Delivering Healthcare in America Chapter 8 Review Questions 6th Edition
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
5
The Health Care Delivery System
For Americans to enjoy optimal health—as individuals and as a population—they must have the benefit of high-quality health care services that are effectively coordinated within a strong public health system. In considering the role of the health care sector in assuring the nation's health, the committee took as its starting point one of the recommendations of the Institute of Medicine (IOM) report Crossing the Quality Chasm (2001b: 6): "All health care organizations, professional groups, and private and public purchasers should adopt as their explicit purpose to continually reduce the burden of illness, injury, and disability, and to improve the health and functioning of the people of the United States."
This chapter addresses the issues of access, managing chronic disease, neglected health care services (i.e., clinical preventive services, oral, and mental health care and substance abuse services), and the capacity of the health care delivery system to better serve the population in terms of cultural competence, quality, the workforce, financing, information technology, and emergency preparedness. In addition, the chapter discusses the responsibility of the health care system to recognize and play its appropriate role within the intersectoral public health system, particularly as it collaborates with the governmental public health agencies.
The health care sector in the United States consists of an array of clinicians, hospitals and other health care facilities, insurance plans, and purchasers of health care services, all operating in various configurations of groups, networks, and independent practices. Some are based in the public sector; others operate in the private sector as either for-profit or not-for-
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
profit entities. The health care sector also includes regulators, some voluntary and others governmental. Although these various individuals and organizations are generally referred to collectively as "the health care delivery system," the phrase suggests an order, integration, and accountability that do not exist. Communication, collaboration, or systems planning among these various entities is limited and is almost incidental to their operations. For convenience, however, the committee uses the common terminology of health care delivery system.
As described in Crossing the Quality Chasm (IOM, 2001b) and other literature, this health care system is faced with serious quality and cost challenges. To support the system, the United States spends more per capita on health care than any other country ($4,637 in 2000) (Reinhardt et al., 2002). In the aggregate, these per capita expenditures account for 13.2 percent of the U.S. gross domestic product, about $1.3 trillion (Levit et al., 2002). As the committee observed in Chapter 1, American medicine and the basic and clinical research that inform its practice are generally acknowledged as the best in the world. Yet the nation's substantial health-related spending has not produced superlative health outcomes for its people. Fundamental flaws in the systems that finance, organize, and deliver health care work to undermine the organizational structure necessary to ensure the effective translation of scientific discoveries into routine patient care, and many parts of the health care delivery system are economically vulnerable. Insurance plans and providers scramble to adapt and survive in a rapidly evolving and highly competitive market; and the variations among health insurance plans—whether public or private—in eligibility, benefits, cost sharing, plan restrictions, reimbursement policies, and other attributes create confusion, inequity, and excessive administrative burdens for both providers of care and consumers.
Because of its history, structure, and particularly the highly competitive market in health services that has evolved since the collapse of health care reform efforts in the early 1990s, the health care delivery system often does not interact effectively with other components of the public health system described in this report, in particular, the governmental public health agencies. Health care's structure and incentives are technology and procedure driven and do not support time for the inquiry and reflection, communication, and external relationship building typically needed for effective disease prevention and health promotion. State health departments often have legal authority to regulate the entry of providers and purchasers of health care into the market and to set insurance reimbursement rates for public and, less often, private providers and purchasers. They may control the ability of providers to acquire desired technology and perform complex, costly procedures that are important to the hospital but increase demands on state revenues. Finally, virtually all states have the legal responsibility to
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
monitor the quality of health services provided in the public and private sectors. Many health care providers argue that such regulation adds to their costs, and high-profile problems can create additional tensions that impede collaboration between the state public health agency and the health care delivery system.
Furthermore, when the delivery of health care through the private sector falters, the responsibility for providing some level of basic health care services to the poor and other special populations falls to governmental public health agencies as one of their essential public health services, as discussed in Chapter 1. In many jurisdictions, this default is already occurring, consuming resources and impairing the ability of governmental public health agencies to perform other essential tasks.
Although this committee was not constituted to investigate or make recommendations regarding the serious economic and structural problems confronting the health care system in the United States, it concluded that it must examine certain issues having serious implications for the public health system's effectiveness in promoting the nation's health. Drawing heavily on the work of other IOM committees, this chapter examines the influence that health insurance exerts on access to health care and on the range of care available, as well as the shortcomings in the quality of services provided, some of the constraints on the capacity of the health care system to provide high-quality care, and the need for better collaboration within the public health system, especially among governmental public health agencies and the organizations in the personal health care delivery system.
ACCESS TO HEALTH CARE
Health care is not the only, or even the strongest, determinant of health, but it is very important. For most Americans, having health insurance— under a private plan or through a publicly financed program—is a threshold requirement for routine access to health care. "Health insurance coverage is associated with better health outcomes for adults. It is also associated with having a regular source of care and with greater and more appropriate use of health services. These factors, in turn, improve the likelihood of disease screening and early detection, the management of chronic illness, and the effective treatment of acute conditions," IOM notes in a recent report (IOM, 2002a: 6).
Private insurance is predominantly purchased through employment-based groups and to a lesser extent through individual policies (Mills, 2002). Publicly funded insurance is provided primarily through seven government programs (see Table 5–1). Medicare provides coverage to 13.5 percent of the population, whereas Medicaid covers 11.2 percent of the population (Mills, 2002). Additionally, public funding supports directly
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
TABLE 5–1 Government Health Programs
| Program | Year | Enrollment | Expenditures |
| Medicare | 2001 | 40 million aged and disabled individuals a | $242.4 billion h |
| Medicaid | 2002 | 47 million low-income individuals b | $247 billion (federal, $147 billion; state, $100 billion) b |
| SCHIP | 2001 | 4.6 million low-income children c | $4.6 billion c |
| VHA | 2001 | 4.3 million veterans d | $21 billion d |
| IHS | 2001 | 1.5 million American Indians and Alaska Natives e | $3.2 billion e |
| DOD TRICARE | 2001 | 8.4 million active-duty members of the military f | $14.2 billion f |
| FEHBP | 2000 | 9 million federal employees, dependents, and retirees g | $20 billion g |
| NOTE: VHA = Veterans Health Administration; IHS = Indian Health Service; DOD = Department of Defense; FEHBP = Federal Employees Health Benefits Program. SOURCES: a Boards of Trustees (2002). b Smith et al. (2002); CMS (2002a); CMS (2002c). c CMS (2002a); CMS (2002a); CMS (2002c). d GAO (2001b). e IHS (2002a, 2002b). f Department of Defense (2002). g OPM (2001); Office of the President (2001). h DHHS (2002). | |||
delivered health care (through community health centers and other health centers qualified for Medicaid reimbursement) accessed by 11 percent of the nation's uninsured, who constitute 41 percent of patients at such health centers (Markus et al., 2002). Because the largest public programs are directed to the aged, disabled, and low-income populations, they cover a disproportionate share of the chronically ill and disabled. However, they are also enormously important for children. In early 2001, Medicaid and the State Children's Health Insurance Program (SCHIP) provided health care coverage to 23.1 percent of the children in the United States, and this figure had risen to 27.7 percent according to data from the first-quarter estimates in the National Health Interview Survey (NCHS, 2002).
Being uninsured, although not the only barrier to obtaining health care, is by all indications the most significant one. The fact that more than 41 million people—more than 80 percent of whom are members of working families—are uninsured is the strongest possible indictment of the nation's health care delivery system. Those without health insurance or without insurance for particular types of services face serious, sometimes insurmountable barriers to necessary and appropriate care.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Adults without health insurance are far more likely to go without health care that they believe they need than are adults with health insurance of any kind (Lurie et al., 1984, 1986; Berk and Schur, 1998; Burstin et al., 1998; Baker et al., 2000; Kasper et al., 2000; Schoen and DesRoches, 2000). Children without health insurance may be compromised in ways that will diminish their health and productivity throughout their lives.
When individuals cannot access mainstream health care services, they often seek care from the so-called safety-net providers. These providers include institutions and professionals that by mandate or mission deliver a large amount of care to uninsured and other vulnerable populations. People turn to safety-net providers for a variety of reasons: some because they lack health insurance and others because there are no other providers in the area where they live or because language and cultural differences make them uncomfortable with mainstream care. Safety-net providers are also more likely to offer outreach and enabling services (e.g., transportation and child care) to help overcome barriers that may not be directly related to the health care system itself.
In this section, the committee reviews concerns about the barriers to health care that are raised by the lack of health insurance and by threats to the nation's safety-net providers.
The Uninsured and the Underinsured
The persistently large proportion of the American population that is uninsured—about one in five working-age adults and one in seven children— is the most visible and troubling sign of the nation's failure to assure access to health care. Yet the public and many elected officials seem almost willfully ignorant of the magnitude, persistence, and implications of this problem. Surveys conducted over the past two decades show a consistent underestimation of the number of uninsured and of trends in insurance coverage over time (Blendon et al., 2001). The facts about uninsurance in America are sobering (see Box 5–1). By almost any metric, uninsured adults suffer worse health status and live shorter lives than insured adults (IOM, 2002a).
Because insurance status affects access to secure and continuous care, it also affects health, leading to an estimated 18,000 premature deaths annually (IOM, 2002a). Having a regular source of care improves chances of receiving personal preventive care and screening services and improves the management of chronic disease. When risk factors, such as high blood pressure, can be identified and treated, the chances of developing conditions such as heart disease can be reduced. Similarly, if diseases can be detected and treated when they are still in their early stages, subsequent rates of morbidity and mortality can often be reduced. Without insurance, the chances of early detection and treatment of risk factors or disease are low.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–1 Findings from Coverage Matters
In its report Coverage Matters, the IOM Committee on the Consequences of Uninsurance (IOM, 2001a) found the following:
-
Forty-two million people in the United States lacked health insurance coverage in 1999 (Mills, 2000). This number represented about 15 percent of the total population of 274 million persons at that time and 17 percent of the population younger than 65 years of age; 10 million of the uninsured are children under the age of 18 (about 14 percent of all children), and about 32 million are adults between the ages of 18 and 65 (about 19 percent of all adults in this age group).
-
Nearly 3 out of every 10 Americans, more than 70 million people, lacked health insurance for at least a month over a 36-month period. These numbers are greater than the combined populations of Texas, California, and Connecticut.
-
More than 80 percent of uninsured children and adults under the age of 65 lived in working families. Contrary to popular belief, recent immigrants accounted for a relatively small proportion of the uninsured (less than one in five).
-
Insurance status is a powerful determinant of access to care: people without insurance generally have reduced access. Research consistently finds that persons without insurance are less likely to have any physician visits within a year, have fewer visits annually, and are less likely to have a regular source of care. Children without insurance are three times more likely than children with Medicaid coverage to have no regular source of care.
-
The uninsured were less likely to receive health care services, even for serious conditions. Research consistently finds that persons without insurance are less likely to have any physician visits within a year, have fewer visits annually, and are less likely to have a regular source of care (15 percent of uninsured children do not have a regular provider, whereas just 5 percent of children with Medicaid do not have a regular provider), and uninsured adults are more than three times as likely to lack a regular source of care.
However, even when the uninsured receive care, they fare less well than the insured. The IOM Committee on the Consequences of Uninsurance found that "[u]ninsured adults receive health services that are less adequate and appropriate than those received by patients who have either public or private health insurance, and they have poorer clinical outcomes and poorer overall health than do adults with private health insurance" (IOM, 2002a: 87). For example, Hadley and colleagues (1991) found that uninsured adult hospital inpatients had a significantly higher risk of dying in the hospital than their privately insured counterparts. Emergency and trauma care were also found to vary for insured and uninsured patients. Uninsured persons with traumatic injuries were less likely to be admitted to the hospital,
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
received fewer services when admitted, and were more likely to die than insured trauma victims (Hadley et al., 1991).
For children, too, being uninsured tends to reduce access to health care and is associated with poorer health. The 1998 IOM report America's Children: Health Insurance and Access to Care found that uninsured children "are more likely to be sick as newborns, less likely to be immunized as preschoolers, less likely to receive medical treatment when they are injured, and less likely to receive treatment for illness such as acute or recurrent ear infections, asthma and tooth decay" (IOM, 1998:3). That report emphasized that untreated health problems can affect children's physical and emotional growth, development, and overall health and well-being. Untreated ear infections, for example, can have permanent consequences of hearing loss or deafness.
Even when insured, limitations on coverage may still impede people's access to care. Many people who are counted as insured have very limited benefits and are exposed to high out-of-pocket expenses or service restrictions. Three areas in which benefits are frequently circumscribed under both public and private insurance plans are preventive services, behavioral health care (treatment of mental illness and addictive disorders), and oral health care. When offered, coverage for these services often carries limits that are unrelated to treatment needs and are stricter than those for other types of care (King, 2000). Cost-sharing requirements for these services may also be higher than those for other commonly covered services. (Additional discussion of these and other "neglected" forms of care appears later in this chapter.)
Access to care for the insured can also be affected by requirements for cost sharing and copayments. Cost sharing is an effective means to reduce the use of health care for trivial or self-limited conditions. Numerous studies, starting with the RAND Health Insurance Experiment, show that copayments also reduce the use of preventive and primary care services by the poor, although not by higher-income groups (Solanki et al., 2000). The same effects have been shown for the use of behavioral health care services (Wells et al., 2000).
As a result of the nation's increased awareness of bioterrorist threats, there are concerns about the implications of copayments and other financial barriers to health care. Cost sharing may discourage early care seeking, impeding infectious disease surveillance, delaying timely diagnosis and treatment, and posing a threat to the health of the public. The committee encourages health care policy makers in the public and private sectors to reexamine these issues in light of the concerns about bioterrorism.
This committee was not constituted to make specific recommendations about health insurance. The issues are complex, and the failures of health
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
care reform efforts over the past 30 years testify to the difficulty of crafting a solution. However, the committee finds that both the scale of the problem and the strong evidence of adverse health effects from being uninsured or underinsured make a compelling case that the health of the American people as a whole is compromised by the absence of insurance coverage for so many. Assuring the health of the population in the twenty-first century requires finding a means to guarantee insurance coverage for every person living in this country.
Adequate population health cannot be achieved without making comprehensive and affordable health care available to every person residing in the United States. It is the responsibility of the federal government to lead a national effort to examine the options available to achieve stable health care coverage of individuals and families and to assure the implementation of plans to achieve that result.
Safety-Net Providers
Absent the availability of health insurance, the role of the safety-net provider is critically important. Increasing their numbers and assuring their viability can, to some degree, improve the availability of care. The IOM Committee on the Changing Market, Managed Care and the Future Viability of Safety Net Providers defined safety-net providers as "[t]hose providers that organize and deliver a significant level of health care and other health-related services to uninsured, Medicaid, and other vulnerable patients" (IOM, 2000a: 21). That committee further identified core safety-net providers as having two distinguishing characteristics: "(1) by legal mandate or explicitly adopted mission they maintain an 'open door,' offering access to services to patients regardless of their ability to pay; and (2) a substantial share of their patient mix is uninsured, Medicaid, and other vulnerable patients" (IOM, 2000a: 3).
The organization and delivery of safety-net services vary widely from state to state and community to community (Baxter and Mechanic, 1997). The safety net consists of public hospital systems; academic health centers; community health centers or clinics funded by federal, state, and local governmental public health agencies (see Chapter 3); and local health departments themselves (although systematic data on the extent of health department services are lacking) (IOM, 2000a). A recent study of changes in the capacities and roles of local health departments as safety-net providers found, however, that more than a quarter of the health departments surveyed were the sole safety-net providers in their jurisdictions and that this was more likely to be the case in smaller jurisdictions (Keane et al., 2001).
Safety-net service providers, which include local and state governmen
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
tal agencies, contribute to the public health system in multiple ways. Services provided by state and local governments often include mental health hospitals and outpatient clinics, substance abuse treatment programs, maternal and child health services, and clinics for the homeless. In addition, an estimated 1,300 public hospitals nationwide (Legnini et al., 1999) provide free care to those without insurance or resources to pay. A survey of 69 hospitals belonging to the National Association of Public Hospitals indicated that in 1997, public hospitals provided more than 23 percent of the nation's uncompensated hospital care (measured as the sum of bad debt and charity care) (IOM, 2000a). These demands can overwhelm the traditional population-oriented mission of the governmental public health agencies. Furthermore, changes in the funding streams or reimbursement policies for any of these programs or increases in demand for free or subsidized care that inevitably occur in periods of economic downturn create crises for safety-net providers, including those operated by state and local governments (see the section Collaboration with Governmental Public Health Agencies later in this chapter for additional discussion).
The IOM committee that produced the report America's Health Care Safety Net: Intact but Endangered (IOM, 2000a: 205–206) had the following findings:
The committee fully endorses the recommendations from America's Health Care Safety Net: Intact but Endangered (IOM, 2000a), aimed at ensuring the continued viability of the health care safety net (see Box 5–2).
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–2 Recommendations Concerning Safety-Net Services
-
Federal and state policy makers should explicitly take into account and address the full impact (both intended and unintended) of changes in Medicaid policies on the viability of safety-net providers and the populations they serve.
-
All federal programs and policies targeted to support the safety net and the populations it serves should be reviewed for their effectiveness in meeting the needs of the uninsured.
-
Concerted efforts should be directed to improving this nation's capacity and ability to monitor the changing structure, capacity, and financial stability of the safety net to meet the health care needs of the uninsured and other vulnerable populations.
-
Given the growing number of uninsured people, the adverse effects of Medicaid managed care on safety-net provider revenues, and the absence of concerted public policies directed at increasing the rate of insurance coverage, the committee believes that a new targeted federal initiative should be established to help support core safety-net providers that care for a disproportionate number of uninsured and other vulnerable people.
SOURCE: IOM (2000a).
NEGLECTED CARE
The committee is concerned that the specific types of care that are important for population health—clinical preventive services, mental health care, treatment for substance abuse, and oral health care—are less available because of the current organization and financing of health care services. Many forms of publicly or privately purchased health insurance provide limited coverage, and sometimes no coverage, for these services.
Clinical Preventive Services
The evidence that insurance makes a difference in health outcomes is well documented for preventive, screening, and chronic disease care (IOM, 2002b). Clinical preventive services are the "medical procedures, tests or counseling that health professionals deliver in a clinical setting to prevent disease and promote health, as opposed to interventions that respond to patient symptoms or complaints" (Partnership for Prevention, 1999:3). Such services include immunizations and screening tests, as well as counseling aimed at changing the personal health behaviors of patients long before
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
clinical disease develops. The importance of counseling and behavioral interventions is evident, given the influence on health of factors such as tobacco, alcohol, and illicit drug use; unsafe sexual behavior; and lack of exercise and poor diets. These risk behaviors are estimated to account for more than half of all premature deaths; smoking alone contributes to one out of five deaths (McGinnis and Foege, 1993).
Coverage of clinical preventive services has increased steadily over the past decade. In 1988, about three-quarters of adults with employment-based health insurance had a benefit package that included adult physical examinations. Two years later, the proportion had risen to 90 percent (Rice et al., 1998; Kaiser Family Foundation and Health Research and Educational Trust, 2000). The type of health plan is the most important predictor of coverage (RWJF, 2001). The use of financial incentives and data-driven performance measurement strategies to improve physicians' delivery of services such as immunizations (IOM, 2002c) may account for the fact that managed care plans tend to offer the most comprehensive coverage of clinical preventive services and traditional indemnity plans tend to offer the least comprehensive coverage.
Although the trend toward inclusion of clinical preventive services is positive, such benefits are still limited in scope and are not well correlated with evidence regarding the effectiveness of individual services. The U.S. Preventive Services Task Force (USPSTF), a panel of experts convened by the U.S. Public Health Service, has endorsed a core set of clinical preventive services for asymptomatic individuals with no known risk factors. In the committee's view, this guidance to clinicians on the services that should be offered to specific patients should also inform the design of insurance plans for coverage of age-appropriate services. However, the USPSTF recommendations have had relatively little influence on the design of insurance benefits, and recommended counseling and screening services are often not covered and, consequently, not used (Partnership for Prevention, 2001) (see Box 5–3). As might be expected, though, adults without health insurance are the least likely to receive recommended preventive and screening services or to receive them at the recommended frequencies (Ayanian et al., 2000).
Having any health insurance, even without coverage for any preventive services, increases the probability that an individual will receive appropriate preventive care (Hayward et al., 1988; Woolhandler and Himmelstein, 1988; Hsia et al., 2000). Studies of the use of preventive services by Hispanics and African Americans find that health insurance is strongly associated with the increased receipt of preventive services (Solis et al., 1990; Mandelblatt et al., 1999; Zambrana et al., 1999; Wagner and Guendelman, 2000; Breen et al., 2001; O'Malley et al., 2001). However, the higher rates of uninsurance among racial and ethnic minorities contribute significantly
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–3 Partnership for Prevention Survey of Employer Support for Preventive Services
-
Counseling to address serious health risks—tobacco use, physical inactivity, risky drinking, poor nutrition—is least likely to be covered by an employer-sponsored health plan. The U.S. Preventive Services Task Force calls these interventions "vitally important."
-
Nearly 90 percent of employers' most popular plans cover well-baby care, whereas less than half cover contraceptive devices or drugs to prevent unwanted births. Yet about half of all pregnancies and nearly a third of all births each year are unintended.
-
One out of five employer-sponsored plans does not cover childhood immunizations, and one out of four does not cover adolescent immunizations although these are among the most cost-effective preventive services.
SOURCE: IOM (2000a).
to their reduced overall likelihood of receiving clinical preventive services and to their poorer clinical outcomes (Haas and Adler, 2001). For example, African Americans and members of other minority groups who are diagnosed with cancer are more likely to be diagnosed at advanced stages of disease than are whites (Farley and Flannery, 1989; Mandelblatt et al., 1991, 1996; Wells and Horm, 1992).
Medicare Coverage of Preventive Services
Preventive services are important for older adults, for whom they can reduce premature morbidity and mortality, help preserve function, and enhance quality of life. Unfortunately, the Medicare program was not designed with a focus on prevention, and the process for adding preventive services to the Medicare benefit package is complex and difficult. Unlike forms of treatment that are incorporated into the payment system on a relatively routine basis as they come into general use, preventive services are subject to a greater degree of scrutiny and a demand for a higher level of effectiveness, and there is no routine process for making such assessments. Box 5–4 lists the preventive services currently covered by Medicare.
The level of use of preventive services among older adults has been relatively low (CDC, 1998). This may reflect the limited range of benefits covered by Medicare, as well as other barriers such as copayments, participants' unfamiliarity with the services, or the failure of physicians to recom
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–4 Preventive Services Covered by Medicare
For individuals with Medicare, the following services are covered by Medicare Part B:
-
Bone mass measurements for people at risk of losing bone mass
-
Colorectal cancer screening (people age 50 and older)
-
Diabetes services (coverage of self-management training and glucose monitoring supplies) for people with diabetes
-
Mammogram screening (women age 40 and older)
-
Pap test and pelvic examination (women)
-
Prostate cancer screening (men age 50 and older)
-
Vaccinations (flu, pneumococcal pneumonia, hepatitis B)
-
Outpatient nutrition counseling by registered dietitians for patients with diabetes and some types of kidney disease
SOURCE: HCFA (2001).
mend them. Cardiovascular disease and diabetes exemplify the problem. Although cardiovascular disease is the leading cause of death and diabetes is one of the most significant chronic diseases affecting Medicare beneficiaries, physicians cannot screen for lipids disorders or diabetes unless the patient agrees to pay out-of-pocket for the tests.
Medicaid Coverage of Preventive Services
Medicaid benefits vary by state in terms of both the individuals who are eligible for coverage and the actual services for which coverage is provided. The exception is preventive services for children. In 1976, the U.S. Congress added the Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) program to the federal Medicaid program. This entitled poor children to a comprehensive package of preventive health care and medically necessary diagnostic and treatment services. In 1996, 22.9 million children (20 percent of the nation's children) were eligible for EPSDT benefits. Given its potential to reach such a high proportion of the nation's neediest children, the program could have a very positive, widespread impact on children's health. Unfortunately, data on the program's progress are incomplete and inconsistent across the country, despite federal requirements for state reports (GAO, 2001a). However, some studies have demonstrated that EPSDT has never been fully implemented, and the percentage of children receiving preventive care through it remains low for reasons ranging from
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
systemic state or local deficiencies (e.g., a lack of mechanisms for follow-up, issues related to managed care contracting, and confusing program requirements) to barriers at the personal level (e.g., transportation and language) (GAO, 2001a; Strasz et al., 2002). Of the 22.9 million children eligible for EPSDT in 1996, only 37 percent received a medical screening procedure through the program (Olson, 1998) (see Box 5–5). Additionally, data show that as many as 50 percent of children who have an EPSDT visit are identified as requiring medical attention, but if they are referred for follow-up care, only one-third to two-thirds go for their referral visit (Rosenbach and Gavin, 1998).
Mental Health Care
The Surgeon General's report on mental illness (DHHS, 1999) estimates that more than one in five adults are affected by mental disorders in any given year (see Box 5–6) and 5.4 percent of all adults have a serious mental illness. Data for children are less reliable, but the overall prevalence of mental disorders is also estimated to be about 20 percent (DHHS, 1999). Mental disorders are a major public health issue because they affect such a large proportion of the population, have implications for other health problems, and impose high costs, both financial and emotional, on affected individuals and their families. The cost to society is also high, with indirect costs from lost productivity for affected individuals and their caretakers estimated at $79 billion in 1990, the last year for which estimates are available (Rice and Miller, 1996).
For the most prevalent mental health disorders such as depression and anxiety, receipt of appropriate care is associated with improved functional outcomes at 2 years (Sturm et al., 1995), but the majority of individuals suffering from mental illness are not treated for their condition (DHHS, 1999). Access to care is constrained by limitations on insurance coverage that are greater than those imposed for other diseases. Annual and lifetime coverage limits are frequently less, and mental health coverage often has more hidden costs in the forms of copayments and higher deductibles (Zuvekas et al., 1998). Table 5–2 shows the distribution of sources of payment for treatment for mental health and addictive disorders in 1996. Additionally, those with no insurance all year paid nearly 60 percent of costs out-of-pocket, whereas those with some private insurance paid 40 percent of costs out-of-pocket in 1996 (Zuvekas, 2001).
Adults' use of mental health services in both the general and the specialty mental health sectors correlates highly with health insurance coverage (Cooper-Patrick et al., 1999; Wang et al., 2000; Young et al., 2001), and health insurance coverage specifically for mental health services is associated with an increased likelihood of receiving such care (Wang et al.,
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–5 Children's Preventive Health Care under Medicaid
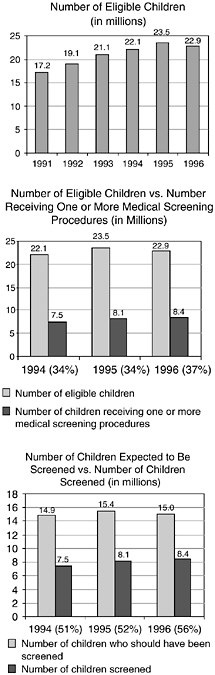
Number of eligible children. Between 1991 and 1996, the number of children eligible for the Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) program increased by roughly 5.7 million, with the highest number (23.5 million children) occurring in 1995. The number of eligible children fell by more than half a million between 1995 and 1996.
Medical screening. Of the 22.9 million children eligible for the EPSDT program in 1996, only 37 percent received a medical screen through the EPSDT program. The medical screening rate is not adjusted according to the federal periodicity schedule or the average period of eligibility, but instead reports the percentage of children who were eligible for any period of time during fiscal year 1996 and who received one or more medical screens. Young children were significantly more likely to be screened: 76 percent of infants under age 1 were screened in 1996, whereas 18 percent of adolescents ages 15 to 20 were screened in 1996.
The participant rate. The participant rate—the number of children screened compared to the number of children expected to be screened, based on the federal periodicity schedule and the average period of eligibility—increased from 51 percent in 1994 to 56 percent in 1996. In 1990, the Health Care Financing Administration established a participant rate goal of 80 percent, to be achieved by fiscal year 1995. As of fiscal year 1996, only nine states reported meeting or exceeding the federally established goal.
SOURCE: Adapted from Olson et al. (1998).
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–6 Facts About Mental Illness
-
About 40 million people (more than one in five) ages 18 to 64 are estimated to have a single mental disorder of any severity or both a mental and an addictive disorder in a given year (Regier et al., 1993; Kessler et al., 1994).
-
The most common conditions fall into the broad categories of schizophrenia, affective disorders (including major depression and bipolar or manic-depressive illness), and anxiety disorders (e.g., panic disorder, obsessive-compulsive disorder, posttraumatic stress disorder, and phobia).
-
Schizophrenia affects at least an estimated 2 million Americans in any year (Regier et al., 1993), whereas the most prevalent affective disorder, major depression, has been reported to occur in 6.5 percent of women and 3.3 percent of men in any year (DHHS, 2000a). Manic-depressive illness is reported to exist in 1 percent of adults. Anxiety disorders affect an estimated 19 million Americans annually (DHHS, 2000a).
-
Only 25 percent of people who have a mental disorder obtain diagnosis and treatment from the health care system, in contrast to 60 to 80 percent of those with heart disease (DHHS, 2000a).
-
Evidence-based practice guidelines for depression endorse antidepressant medications and cognitive-behavioral or interpersonal psychotherapies (AHCPR, 1993; Department of Veterans Affairs, 1993; Schulberg et al., 1999).
SOURCE: IOM (2002b).
2000; Young et al., 2000). Recent studies have shown impressive results for treatment of depression in primary care settings (Sturm and Wells, 2000; Schoenbaum et al., 2001). The provision of such services is cost-effective and comparable to the cost-effectiveness of other common procedures. However, reimbursement policies for primary care do not support the services necessary to provide evidence-based care for depression (Wells et al., 2000; Schoenbaum et al., 2001).
Adults with either no insurance coverage or coverage that excludes or limits extended treatment of mental illness receive less appropriate care and may experience delays in receiving services until they gain public insurance (Rabinowitz et al., 2001). Adults with mental disorders are also more likely to lose health insurance coverage within a year following their diagnosis than those without a mental disorder (Sturm and Wells, 2000).
The limited and unstable nature of insurance for treatment of mental illness has several implications for governmental public health agencies because the severely mentally ill are likely to end up receiving care in publicly funded safety-net programs (Rabinowitz et al., 2001). Funding to support the public mental health system comes from reimbursements for
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
TABLE 5–2 Distribution (percent) of Sources of Payment for Mental Health/Substance Abuse Treatment, by Type of Use, 1996
| Payment Source | Total | Ambulatory Care | Psychotropic Medications | Inpatient Care |
| Total | ||||
| Out-of-pocket | 23.0 | 32.4 | 39.1** | — a |
| Private | 39.4 | 34.3 | 42.1** | 43.8 |
| Medicaid | 19.6 | 19.5 | 16.2* | 21.7 |
| Medicare | 14.3** | 7.4** | — a | 30.0* |
| Other public | 02.0** | 3.7** | 01.7** | — a |
| Other | — a | — a | — a | — a |
| a Relative standard error is too large to support reliable estimation. *p < .10 **p < .05 SOURCE: Zuvekas (2001), based on the 1996 Medical Expenditure Panel Survey. | ||||
services provided to Medicare and Medicaid participants, from federal block grants to states, and from state and local funds that support community-based programs and hospital care. Taken in the aggregate, these funding streams are neither adequate nor reliable enough to meet the needs of individuals with serious mental disorders (IOM, 2000a). As with other forms of safety-net care, the urgency of providing treatment to the severely mentally ill erodes funds available for prevention purposes.
Treatment for Substance Abuse
In the United States, more than 18 million people who use alcohol and nearly 5 million who use illicit drugs need substance abuse treatment (SAMHSA, 2001). Substance abuse, like mental illness, exacts enormous social costs across all segments of society. The total social costs of alcohol abuse alone were estimated at $177.3 billion in 1997 (Coffey et al., 2001). In that same year, $6.4 billion was spent on treatment. Total spending on drug abuse treatment equaled $5.5 billion in that year, compared with estimated social costs of drug abuse of $116.9 billion.
Most recipients (87 percent) of specialty treatment for alcohol or drug abuse receive it in outpatient settings (RWJF, 2001), but overall, less than one-fourth of those who need treatment get it. Barriers to treatment include stigma, lack of available treatment facilities, unwillingness to admit that treatment is needed, and inability to pay for care. Public sources provide more than two-thirds of the funding for alcohol and drug treatment facilities. Half of such funds come from dedicated funding at the federal, state, and local levels in the form of various block grants to state safety-net programs.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Medicaid and Medicare cover 21 percent of treatment, private insurance covers 14 percent, and 10 percent is paid directly by patients as out-of-pocket costs. Another 5 percent is covered through various charitable sources.
Insurance policies held by many individuals constrain the use of substance abuse services by the exclusion of benefits for such services and by the use of annual and lifetime limits on benefits and other controls on service utilization. Between 1987 and 1997, private insurance for substance abuse services fell 0.2 percent per year on average (inflation adjusted). Over the same period, out-of-pocket payments for specific types of substance abuse treatment increased (Coffey et al., 2001). However, the high out-of-pocket costs faced by individuals who pay for their own treatment discourage many who need care from seeking it.
Oral Health Care
Like mental illness and addiction disorders, oral health has been neglected in the health care delivery system. The consequences in terms of individual and population health are significant—oral health is a matter of public health concern because it affects a large proportion of the population and is linked with overall health status (see Box 5–7). Oral diseases are causally related to a range of significant health problems and chronic diseases, as well as individuals' ability to succeed in school, work, and the community (DHHS, 2000b). The effects of oral diseases are cumulative and influence aspects of life as fundamental as the foods people can eat, their ability to communicate effectively, and their social acceptability. The problems in the way the health care delivery system relates to oral health include lack of dental coverage and low coverage payments, the separation of medicine and dentistry in training and practice, and the high proportion of the population that lacks any dental insurance. The committee focused on the problem of insurance and access to care.
According to the Department of Health and Human Services (DHHS) Office of Health Promotion and Disease Prevention, more than 150 million Americans have limited or no dental insurance, nearly four times the number who lack insurance for medical care (cited by Allukian, 1999). As with other types of health services, insurance is a strong predictor of access to and use of dental services, and minorities and low-income populations are much less likely to have dental insurance or to receive dental care.
Individuals and families living below the poverty level experience more dental decay than higher-income groups, and their cavities are less likely to be treated (GAO, 2000). More than a third of poor children (ages 2 to 9) have one or more primary teeth with untreated decay, compared with 17.3 percent of nonpoor children (DHHS, 2000b). Mexican-American adults and children are more likely to have untreated decayed teeth than any other
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–7 Oral Health as a Component of Total Health
When people think about the components of good health, they often forget about the importance of good oral health. This oversight is often reflected by health insurance coverage restrictions that exclude oral health care.
Oral health is important because the condition of the mouth is often indicative of the condition of the body as a whole. More than 90 percent of systemic diseases have oral manifestations. These diseases include immune deficiency (e.g., HIV/ AIDS), viral diseases (e.g., herpes and mumps), cancer and leukemia, diabetes, heart disease, kidney disease, anemia, hemophilia and other bleeding disorders, adrenal gland disorders, and inflammatory bowel disease (Bajuscak, 1999; Glick, 1999). Also, poor oral health can lead to poor general health. Infections in the mouth can enter the bloodstream and affect the functioning of major organs (e.g., bacterial endocarditis, in which infection causes the lining of the heart and the heart valves to become inflamed) (Meadows, 1999). Poor oral care can also contribute to oral cancer, and untreated tooth decay can lead to tooth abscess, tooth loss, and—in the worst cases—serious destruction of the jawbone (Meadows, 1999).
For these reasons, oral health must recognized as an important component of assuring individual and population health. The awareness that the mouth may be a mirror to the body can help to prevent illness, diagnose serious conditions early, and maintain optimum overall health (Glick, 1999).
population group. Poor Mexican-American children ages 2 to 9 have the highest proportion of untreated decayed teeth (70.5 percent), followed by poor non-Hispanic African-American children (67.4 percent). The pattern for adults is similar (DHHS, 2000b: 63–64).
Medicare excludes coverage of routine dental care, and many state Medicaid programs do not provide dental coverage for eligible children or adults. According to a report of the Surgeon General, fewer than one in five Medicaid-covered children received a single dental visit in a recent year-long study period (DHHS, 2000b). Low-income Hispanic children and adults are less likely to be eligible for Medicaid than other groups, so even the limited Medicaid benefits are unlikely to be available to them. The forecast for major oral health problems among the nation's fastest-growing population group, Hispanics, is especially alarming.
The committee found that preventive, oral health, mental health, and substance abuse treatment services must be considered part of the comprehensive spectrum of care necessary to help assure maximum health. Therefore, the committee recommends that all public and privately funded insurance plans include age-appropriate preventive services as recommended by
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
the U.S. Preventive Services Task Force and provide evidence-based coverage of oral health, mental health, and substance abuse treatment services.
PROBLEMS IN QUALITY OF CARE
Crossing the Quality Chasm (IOM, 2001b) examined health system failures that compromise the quality of care provided to all Americans. As noted, it is often the responsibility of state departments of health to monitor providers and levy sanctions when quality problems are identified. This adds to potential tensions with the public health system. Two particular quality problems have special significance in terms of assuring the health of the population: disparities in the quality of care provided to racial and ethnic minorities and inadequate management of chronic diseases. As the American population grows both older and more racially and ethnically diverse and as rates of chronic disease increase, important vulnerabilities in the health care delivery system are compromising individual and population health (Murray and Lopez, 1996; Hetzel and Smith, 2001).
Disparities in Health Care
A principal finding from Crossing the Quality Chasm (IOM, 2001b: 53) is that "the quality of care should not differ because of such characteristics as gender, race, age, ethnicity, income, education, disability, sexual orientation, or place of residence." Disparities in health care are defined as "racial or ethnic differences in the quality of health care that are not due to access-related factors or clinical needs, preferences and appropriateness of intervention" (IOM, 2002b: 4).
Evidence shows that racial and ethnic minorities do not receive the same quality of care afforded white Americans. These findings are consistent across a range of illnesses and health care services and remain even after adjustment for socioeconomic differences and other factors that are related to access to health care (IOM, 2002b). Furthermore, poor-quality health care is an important independent variable contributing to lower health status for minorities (IOM, 2002b). For example, racial differences in cervical cancer deaths have increased over time, despite the greater use of screening tests by minority women (Mitchell and McCormack, 1997). The lower quality of care also compounds the adverse health effects of other disadvantages faced by minorities, including lower incomes and education, less healthy living environments, and a greater likelihood of being uninsured.
As discussed in Unequal Treatment (IOM, 2002b), the factors that may produce disparities in health care include the role of bias, discrimination, and stereotyping at the individual (provider and patient), institution, and
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
health system levels. The report found that aspects of the health care system—its organization, financing, and availability of services—may have adverse effects specifically for racial and ethnic minorities. For example, time pressures on physicians hamper their ability to accurately assess presenting symptoms, especially when cultural or language barriers are present. Nearly 14 million people in the United States are not proficient in English.
Changes in the financing and delivery of health care services, such as the emphasis on cost controls and the almost complete conversion to managed care for the delivery of services under Medicaid, may be especially problematic for racial and ethnic minorities. The disruption of traditional community-based care and the displacement of providers who are familiar with the language, culture, and values of ethnic communities create barriers to effective care (Leigh et al., 1999). In addition, segmentation of health care plans was found to play a significant role in producing poorer care for racial and ethnic minorities because they are more likely than whites to be enrolled in "lower-end" health plans (IOM, 2002b). Such plans are characterized by higher per capita resource constraints and stricter limits on covered services (Phillips et al., 2000). Fragmentation of health plans along socioeconomic lines engenders different clinical cultures, with different practice norms (Bloche, 2001).
The committee encourages the health care system and policy makers in the public and private sectors to give careful consideration to the interventions that are identified in Unequal Treatment (IOM, 2002b) and aimed at eliminating racial and ethnic disparities in health care (see Box 5–8).
Care for Chronic Conditions
Americans now live longer. A child born today can expect to live more than 75 years, and advances in medicine have also extended the life spans of earlier generations. As detailed in Chapter 1, the result is that individuals over age 65 constitute an increasingly large proportion of the U.S. population—13 percent today, increasing to 20 percent over the next decade. Embedded in these demographic changes is a dramatic increase in the prevalence of chronic conditions. Chronic conditions, defined as illnesses that last longer than 3 months and that are not self-limiting, affect nearly half of the U.S. population. An estimated 100 million Americans have one or more chronic conditions, and that number is estimated to reach 134 million by 2020 (Pew Environmental Health Commission, 2001). Nearly half of those with a chronic illness have more than one such condition (IOM, 2001a). Additionally, disabling chronic conditions affect all age groups, but about two-thirds are found in individuals over age 65. With the projected growth in the number of people over age 65 increasing from 13 percent of the
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–8 Legal, Regulatory, and Policy Interventions to Eliminate Racial and Ethnic Disparities in Health Care
-
Avoid fragmentation of health plans along socioeconomic lines.
-
Strengthen the stability of patient–provider relationships in publicly funded health plans.
-
Increase the proportion of underrepresented U.S. racial and ethnic minorities among health professionals.
-
Apply the same managed care protections to publicly funded health maintenance organization (HMO) enrollees that apply to private HMO enrollees.
-
Provide greater resources to the Department of Health and Human Services Office of Civil Rights to enforce civil rights laws.
-
Promote the consistency and equity of care through the use of evidence-based guidelines.
-
Structure payment systems to ensure an adequate supply of services to minority patients and limit provider incentives that may promote disparities.
-
Enhance patient–provider communications and trust by providing financial incentives for practices that reduce barriers and encourage evidence-based practice.
-
Support the use of interpretation services where community need exists.
-
Support the use of community health workers.
-
Implement multidisciplinary treatment and preventive care teams.
-
Implement patient education programs to increase patients' knowledge of how to best access care and participate in treatment decisions.
-
Integrate cross-cultural education into the training of all current and future health care professionals.
-
Collect and report data on health care access and utilization by patients' race, ethnicity, socioeconomic status, and, where possible, primary language.
SOURCE: IOM (2002c).
population to 20 percent, the need for care for chronic conditions will also continue to grow.
As detailed in Crossing the Quality Chasm (IOM, 2001b: 27), effective health care for chronic disease management is a collaborative process, involving the "definition of clinical problems in terms that both patients and providers understand; joint development of a care plan with goals, targets, and implementation strategies; provision of self-management training and support services; and active, sustained follow-up using visits, telephone calls, e-mail, and Web-based monitoring and decision support systems."
The current health care system does not meet the challenge of providing clinically appropriate and cost-effective care for the chronically ill. Crossing the Quality Chasm (IOM, 2001b: 28) found that "the prevailing model of
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
health care delivery is complicated, comprising layers of processes and handoffs that patients and families find bewildering and clinicians view as wasteful . . . a nightmare to navigate." Although this reality is a challenge for anyone seeking care, the effects become especially damaging for those with chronic conditions. Wagner and colleagues (1996) identified five elements required to improve outcomes for chronically ill patients:
-
Evidence-based planned care.
-
Reorganization of practices to meet the needs of patients who require more time, a broad array of resources, and closer follow-up.
-
Systematic attention to patients' need for information and behavioral change.
-
Ready access to necessary clinical expertise.
-
Supportive information systems.
The health care delivery system as it exists today cannot deliver those elements. Recent surveys have found that less than half of U.S. patients with hypertension, depression, diabetes, and asthma are receiving appropriate treatments (Wagner et al., 2001). Delivery of high-quality care to chronically ill patients is especially challenging in a decentralized and fragmented system, characterized by small practices (AMA, 1998). Smaller practices have great difficulty in organizing the array of services and support needed to efficiently manage chronic disease. The result is poor disease management and a high level of wasted resources. As the proportion of old and very old increases, the system-wide impact in terms of cost and increased disability may well overwhelm the human and financial resources available to care for chronically ill patients.
CAPACITY OF THE HEALTH CARE SYSTEM TO SERVE THE POPULATION
The resources of the health care delivery system are not balanced well enough to provide patient-centered care, to address the complex health care demands of an aging population, to absorb normal spikes in demand for urgent care, and to manage a large-scale emergency such as that posed by a terrorist attack. The relentless focus on controlling costs over the past decade has squeezed a great deal of excess capacity out of the health care system, particularly the hospital system. It has also reduced the time that physicians spend with patients and the quality of the clinical encounter. At the same time, the design of insurance plans (in both the public and the private sectors) does not support the integrated disease management protocols needed to treat chronic disease or the data gathering and analysis needed for both disease management and population-level health. Underly
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
ing all of these problems is the absence of a national health information infrastructure to support research, clinical medicine, and population-level health.
Shortages of Health Care Professionals
The committee took special note of certain shortages of health care professionals, because these shortages are having a significant adverse effect on the quality of health care. The committee's particular concerns are the underrepresentation of racial and ethnic minorities in all health professions and the shortage of nurses, especially registered nurses (RNs) practicing in hospitals.
However, the focus on these two health care professional shortage areas does not suggest the absence of problems in other fields. Acute shortages of primary care physicians exist in many geographic areas, in certain medical specialties, and in disciplines such as pharmacy and dentistry, to name two. In addition, a growing consensus suggests that major reforms are needed in the education and training of all health professionals. To deliver the type of health care envisioned in Crossing the Quality Chasm (IOM, 2001b), health care professionals must be trained to work in teams, to utilize information technology effectively, and to develop the competencies necessary to deliver care to an increasingly diverse population. Health professions education is not currently organized to produce these results.
Underrepresentation of Racial and Ethnic Minorities
In 2000, 9 percent of physicians and 12.3 percent of RNs were from racial and ethnic minority groups (AAMC, 2000). By comparison, racial and ethnic minorities account for more than one-quarter of the nation's population. Among physicians, about 3 percent are African American, 2.2 percent are Hispanic, and 3.6 percent are Asian (AAMC, 2000). The 2000 National Sample Survey of Registered Nurses reported that 5 percent of RNs are African American, 2 percent are Hispanic, and 3.5 percent are Asian (Spratley et al., 2000). The severe underrepresentation of racial and ethnic minorities in the health professions affects access to care for minority populations, the quality of care they receive, and the level of confidence that minority patients have in the health care system.
A consistent body of research indicates that African-American and Hispanic physicians are more likely to provide services in minority and underserved communities and are more likely to treat patients who are poor, Medicaid eligible, and sicker (IOM, 2001c). Some studies indicate that, on average, minority physicians treat four to five times more minority patients than do white physicians, and studies of recent minority medical
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
school graduates indicate that they have a greater preference to serve in minority and underserved areas. Although more research is needed to examine the impact of minority health care professionals on the level of access and quality of care, for some minority patients, having a minority physician results in better communication, greater patient satisfaction with care, and greater use of preventive services (IOM, 2002b). Although evidence has not established that increasing the numbers of minority physicians or improving cultural competence per se influences patient outcomes, existing research supports clear policies to increase the proportion of medical students drawn from minority groups.
Hospital Nursing Shortage
RNs work in a variety of settings, ranging from governmental public health agency clinics to hospitals and nursing homes. The majority, however, work in hospitals, although the proportion dropped from 68 percent in 1968 to 59 percent in 2000 (Spratley et al., 2000). Hospitals are facing shortages of RNs, in addition to shortages of pharmacists, laboratory technologists, and radiological technologists. A recent national hospital survey (AHA, 2001b) found that of 168,000 vacant positions, 126,000 were for RN positions. Hospital vacancy rates for RN positions averaged 11 percent across the country, ranging from about 10 percent to more than 20 percent in some states. Nationally, more than one in seven hospitals report a severe shortage of RNs, with more than 20 percent of RN positions vacant. In general, hospitals in rural areas report the highest percentage of vacant positions. The current shortage of RNs, particularly for hospital practice, is a matter of national concern because nursing care is critical to the operation and quality of care in hospitals (Aiken et al., 1994, 2001). In a study analyzing more than 5 million patient discharges from 799 hospitals in 11 states, Needleman and colleagues (2001) consistently found that higher RN staffing levels were associated with a 3 to 12 percent reduction in indicators—including lower rates of urinary tract infections, pneumonia, shock, and upper gastrointestinal bleeding and shorter lengths of stay—that reflect better inpatient care.
The shortage of hospital-based nurses reflects several factors, including the aging of the population, declining nursing school enrollment numbers (Sherer, 2001), the aging of the nursing workforce (the average age increased from 43.1 years in 1992 to 45.2 years in 2000) (Spratley et al., 2000), and dissatisfaction among nurses with the hospital work environment. Furthermore, nurses have available other professional opportunities, and women, who once formed the bulk of the nursing workforce, now have alternate career prospects. These trends do not appear to be a temporary, cyclical phenomenon. The aging of the population means an increase in the
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
number of patients who require skilled care for chronic diseases and age-related conditions, but the growth in the pool of nursing professionals is not keeping pace with the growth in the patient population.
Although some of this increase is to be expected because of the overall aging of the U.S. labor force, the proportion of workers who are age 35 and older is increasing more for RNs than for all other occupations (IOM, 1996). An aging workforce may have implications for patient care if older RNs have less ability to perform certain physical tasks (HRSA, 2001). The shortage of RNs poses a serious threat to the health care delivery system, and to hospitals in particular.
Hospitals and the Capacity for Emergency Response
Hospitals contribute in various ways to assuring the health of the public, particularly by providing acute care services, educating health professionals, serving as a site for research, organizing community health promotion and disease prevention activities, and acting as safety-net providers. However, hospitals play a uniquely important role by serving as the primary source of emergency and highly specialized care such as that in intensive care units (ICUs) and centers for cardiac care and burn treatment.
Recent changes in the structure of the hospital industry, the reimbursement of hospitals by public- and private-sector insurance programs, and nursing shortages have raised questions about the ability of hospitals to carry out these roles. Although the terrorist incidents in the fall of 2001 did not directly test the ability of hospitals to respond to a medical crisis, they drew particular attention to hospitals' limited "surge capacity"—the ability to absorb a large influx of severely injured patients—in their emergency departments and specialty units.
During the 1990s, the spread of managed care practices contributed to reductions in overall hospital admissions, in the length of hospital stays, and in emergency department visits. As a result of decreasing demand for hospital services and a changing financial environment, hospitals in many parts of the country reduced the number of patient beds, eliminated certain services, or even closed (McManus, 2001). The American Hospital Association (AHA, 2001a) reports that from 1994 to 1999, the number of emergency departments in the nation decreased by 8.1 percent (see Table 5–3). Over the same period, medical and surgical bed capacities were reduced by 17.7 percent, ICU bed capacities were reduced by 2.8 percent, and specialty bed (including burn bed) capacities were reduced by 3.4 percent. Although these reductions may have improved the efficiencies of hospitals, they have important implications for the capacity of the health care system to respond to public health emergencies.
Crowding in hospital emergency departments has been recognized as a
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
TABLE 5–3 Change in Hospital Capacity, 1994–1999
| Component | 1994 | 1999 | Percent Change, 1994–1999 |
| Emergency departments | 4,547 | 4,177 | –8.1 |
| Medical/surgical beds | 533,848 | 439,426 | –17.7 |
| ICU beds | 72,229 | 70,215 | –2.8 |
| Special care beds a | 15,373 | 14,848 | –3.4 |
| Total inpatient beds b | 621,450 | 524,489 | 15.6 |
| a Burn care beds and other special care beds intended for care that is less intensive than that provided in an ICU and more intensive than that provided in an acute care area. b Total of medical and surgical beds, ICU beds, and special care beds. SOURCE: Brewster et al. (2001), citing the American Hospital Association (2001a). | |||
nationwide problem for more than a decade (Andrulis et al., 1991; Brewster et al., 2001; McManus, 2001; Viccellio, 2001). According to the American Hospital Association (2001a), the demand for emergency department care increased by 15 percent between 1990 and 1999. In a random survey of emergency department directors in 1998 and 1999, 91 percent of the 575 respondents reported overcrowding problems (Derlet et al., 2001). The overcrowding was severe, resulting in delays in testing and treatment that compromised patient outcomes. The emergency departments of hospitals in many areas of New York City routinely operated at 100 percent capacity (Brewster et al., 2001). Patients regularly spent significant portions of their admission on gurneys in a hallway.
One consequence of this crowding is the periodic closure of emergency departments and the diversion of ambulances to other facilities. Ambulance diversions have been found to impede access to emergency services in metropolitan areas in at least 22 states (U.S. House of Representatives, 2001); at least 75 million Americans are estimated to reside in areas affected by ambulance diversions. Looking at 12 communities, Brewster and colleagues (2001) found that on average in 2001, two hospitals in Boston closed their emergency departments each day and the Cleveland Clinic emergency departments were closed to patients arriving by ambulance for an average of nearly 12 hours a day.
The increase in demand for emergency care is attributed to several factors (Brewster et al., 2001). In particular, managed care rules have changed to allow increased coverage of care provided in emergency departments. Hospitals are in better compliance with the federal Emergency Medical Treatment and Labor Act, which requires emergency departments to treat patients without regard for their ability to pay. In addition,
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
uninsured patients are making greater use of emergency departments for nonurgent care.
Access to Primary Care
The adequacy of hospital capacity cannot be assessed without considering the system inefficiencies that characterize current insurance and care delivery arrangements. These include the demands placed on hospital emergency and outpatient departments by the uninsured and those without access to a primary care provider. The unique characteristic of primary care is the role it plays as a regular or usual source of care for patients and their families. Good primary care assures continuity for the patient across levels of care, comprehensiveness of services according to the level of health or illness, and better coordination of these services over time (Starfield, 1998).
Defining the right level of immediate and standby capacity for emergency and inpatient care depends in part on the adequacy and effectiveness of general outpatient and primary care. For example, chronic conditions like asthma and diabetes often can be managed effectively on an outpatient basis, but if the conditions are poorly managed by patients or their health care providers, emergency or inpatient care may be necessary. Billings and colleagues (1993) demonstrated strong links between hospital admission rates for such conditions and the socioeconomic and insurance status of the population in an area. For example, admission rates for asthma were 6.4 percent higher in low-income areas than in higher-income areas, with more than 70 percent of the variation explained by household income (Billings et al., 1993). Differences in disease prevalence accounted for only a small portion of the differences in hospitalization rates among low- and high-income areas.
Although Billings and colleagues did not draw conclusions about the causal pathways leading to these higher admission rates, it is likely that the contributing factors include those discussed in this chapter, such as a lack of insurance or a regular source of care and the assignment of Medicaid populations to lower-cost health plans. A follow-up analysis found the situation to be growing worse for low-income populations, as economic pressures, including lower reimbursements rates, higher practice costs, and limitations on payment for diagnostic tests, squeeze providers who have historically delivered care to academic health centers' low-income populations (Billings et al., 1996). Bindman and colleagues (1995) similarly concluded that at the community level, "there is a strong positive association between health care access and preventable hospitalization rates, suggesting that these rates can serve as an indication of access to care." It would be a costly mistake to create additional emergency and inpatient capacity before decompressing demand by improving access to primary care services. Good
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
primary care is associated with better birth weights (Politzer et al., 2001), lower smoking rates, less obesity, and higher rates of seat belt use (Shi et al., 1999) and is a major determinant of receiving preventive services such as blood pressure screening, clinical breast exams, and Pap smears (Bindman et al., 1996). Geographically, areas with higher primary care physician-to-population ratios experience lower total health care costs (Welch et al., 1993; Mark et al., 1996; Franks and Fiscella, 1998; Starfield and Shi, 2002). Additionally, there is evidence that primary care is associated with reduced disparities in health; areas of high income inequality that also had good primary care were less likely to report fair or poor self-rated health (Starfield, 2002). The link between the availability of primary care and better health is also supported by international evidence, which shows that nations that value primary care are likely to have lower mortality rates (all causes; all causes, premature; and cause specific), even when controlling for macro- and micro-level characteristics (e.g., gross domestic product and per capita income) (Macinko et al., in press).
The Unfulfilled Potential of Managed Care
Although Billings and colleagues focused on the preventable demands for hospital care among low-income and uninsured populations, Closing the Quality Chasm (IOM, 2001b) makes clear that the misuse of services also characterizes disease management among insured chronically ill patients.
In the early 1990s, managed care became a common feature of the health care delivery system in the United States. In theory, managed care offers the promise of a population-based approach that can emphasize regular preventive care and other services aimed at keeping a defined group as healthy as possible. These benefits are most easily achieved under a fully capitated, group practice model: patients enroll with a health care organization that is paid a certain amount per member per month to provide all necessary or indicated services to the enrolled population, and physicians are paid a monthly fee or are salaried, which separates payment from the provision of individual services. This model allows a relatively stable enrolled population for whom benefits and services can be customized; knowledge of the global budget within which care is to be delivered; and a salaried workforce in which health care providers have an incentive to keep patients healthy and reduce unnecessary use of services but also have a culture in which they monitor each others' practices and quality of care. For the patient, the model provides comprehensive care, an emphasis on prevention, and low out-of-pocket costs. Kaiser Permanente Medical Group pioneered the model more than 50 years ago on the basis of early experiences providing health care programs for employees of Kaiser industrial
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
companies (e.g., construction, shipyards, steel mills) in the late 1930s and 1940s.1
An important opportunity was lost when insurance companies, health plans and health providers, and the state and federal governments saw managed care primarily as a cost-containment mechanism rather than a population-based approach to delivering comprehensive and effective health care services. Reimbursement rate reductions, restrictions on care and choice of physician, and other aspects of plan management disaffected millions of Americans from the basic concept of managed care. Furthermore, rapid turnover in enrollment, particularly in Medicaid managed care, ruined economic incentives for plans to view their enrollees as a long-term investment. This loss of trust in the idea of managed care is also the loss of a great opportunity to improve quality and restrain costs. Loosely affiliated physician networks have no ability to identify their populations and develop programs specifically based on the epidemiology of the defined group. There is little ability to use data systems, shared protocols, or peer pressure to improve quality and reduce variations in health care practices.
Managed care is undergoing rapid changes, some of which are likely to further undermine its viability. Consumer demands for more choice and greater flexibility are weakening restrictions on access to providers and limitations on services. Physicians are proving more aggressive and successful in their negotiations with plans to decrease constraints, and to date, most employers have been willing to accept the higher costs that result. Employer acceptance may change in the face of double-digit insurance premium increases.
Predicting the next configuration of insurance and plan delivery systems is dangerous in a system undergoing such rapid transition. A number of major insurance plans have announced that they will begin to offer defined-contribution options.2 This may be attractive to employers, whose liability will be defined by a specific premium amount rather than by a specified set of benefits. Consumers will be expected to shop for their own care with a medical spending account coupled with catastrophic benefits for very large expenses. This could significantly undermine the current
| 1 | Group Health of Puget Sound and the Health Insurance Plan of New York were also pioneers in group model health maintenance organizations. |
| 2 | Defined-contribution health care benefits are a new way for employers to provide health care coverage to their employees, while no longer acting as brokers between employees and insurance companies contracted to provide benefits. An employer may choose from several different ways to put money into a health benefits account for each employee and offer the employee a menu of coverage options, with different funding levels and employee financial responsibility for each. |
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
pooling of risk and create incentives for overuse of high-technology services once a deductible for catastrophic benefits has been met. However, such plans have yet to assume a significant role in the insurance market, and few employers offer them as an alternative.
Information Technology
The development of enhanced information technology and its use in hospitals, individual provider practices, and other segments of the health care delivery system are essential for improving the quality of care. Better information technology can also support patients and family caregivers in crucial health decisions, strengthen both personal and population-based prevention efforts, and enhance participation in and coordination with public health activities. (See Chapter 3 for a discussion of the information technology needs of the governmental public health infrastructure.)
Crossing the Quality Chasm (IOM, 2001b) formulated the case that information technology is critical to the redesign of the health care system to achieve a substantial improvement in the quality of care. A strong clinical information infrastructure is a prerequisite to reengineering processes of care; coordinating patient care across providers, plans, and settings and over time; supporting the operation of multidisciplinary teams and the application of clinical support tools; and facilitating the use of performance and outcome measures for quality improvement and accountability.
From the provider perspective, better information systems and more extensive use of information technology could dramatically improve care by offering ready access to complete and accurate patient data and to a variety of information resources and tools—clinical guidelines, decision-support systems, digital prescription-writing programs, and public health data and alerts, for example—that can enhance the quality of clinical decision making. Computer-based systems for the entry of physician orders have been found to have sizable benefits in enhancing patient safety (Bates et al., 1998, 2001; Schiff et al., 2000).
Despite profound growth in clinical knowledge and medical technology, the health care delivery system has been relatively untouched by the revolution in information technology that has transformed other sectors of society and the economy. Many health care settings lack basic computer systems to provide clinical information or support clinical decision making. Even where electronic medical record systems are being implemented, most of those systems remain proprietary products of individual institutions and health plans that are based on standards of specific vendors.
The development and application of interoperable systems and secure information-sharing practices are essential to gain greater benefits from information technology. At present, only a few institutions have had the
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
resources to build integrated information systems that meet the needs of diverse specialties and environments. Those efforts illustrate both the costs involved in developing health information systems and some of the benefits that might be expected. Kaiser Permanente, for example, is investing $2 billion in a web-based system encompassing all of the critical features needed to provide patient-centered, high-quality care: a nationwide clinical information system, a means for patients to communicate with doctors and nurses to seek medical advice, access by clinicians to clinical guidelines and other knowledge resources, and computerized order entry (Krall, 1998).
So far, however, adoption of even common and less costly information technologies has been limited. Only a small fraction of physicians offer e-mail interaction (13 percent, in a 2001 poll), a simple and convenient tool for efficient communication with their patients (Harris Interactive, 2001). Some of the documented reasons for the low level of physician–patient e-mail communication include concerns about lack of reimbursement for this type of service and concerns about confidentiality and liability. These legitimate issues are slowly being addressed in policy and practice, but there is a long way to go if this form of communication is to achieve its potential for improving interactions between patients and providers.
Enhanced information technology also promises to aid patients and the public in other ways. The Internet already offers a wealth of information and access to the most current evidence to help individuals maintain their own health and manage disease. In addition, support groups and interactive programs offer additional approaches to empower consumers. Personalized systems for comprehensive home care may improve outcomes and reduce costs. Medicare's pilot project IdeaTel—Informatics for Diabetes Education and Telemedicine—offers web-based home systems to rural and inner-city diabetics to support home monitoring, customized information, and secure links to providers and to the patients' own medical records (www.dmi.columbia.edu/ideatel/info.html).
Other efforts to build a personal health record (PHR) created or cocreated and controlled by the individual—and instantly available to support treatment in any setting—suggest that the PHR may provide a comprehensive, accurate, and continuous record to support health and health care across the life span (Jones et al., 1999).
A sophisticated health information infrastructure is also important to support public health monitoring and disease surveillance activities. Systems and protocols for linking health care providers and governmental public health agencies are vital for detecting emerging health threats and supporting appropriate decisions by all parties. The committee cautions, however, that systems dedicated to a single use, such as bioterrorism, will not be optimal; systems designed to be comprehensive and flexible will be of greater overall value. Ultimately, such systems should also allow the
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
public to contribute and receive information to get the most complete database possible.
For information technology to transform the health sector as it has banking and other forms of commerce that depend on the accurate, secure exchange of large amounts of information, action must be taken at the national level to develop the National Health Information Infrastructure (NHII) (NRC, 2000). The committee endorses the call by the National Committee on Vital and Health Statistics (NCVHS) (2002) for the nation to build a twenty-first century health support system—a comprehensive, knowledge-based system capable of providing information to all who need it to make sound decisions about health. Such a system can help realize the public interest related to quality improvement in health care and to disease prevention and health promotion for the population as a whole. The rapid development and widespread implementation of an extensive set of standards for technology and information exchange among providers, governmental public health agencies, and individuals are critical.
Nevertheless, as the NCVHS report describes, neither the opportunities nor the barriers to the development of the NHII are related solely to information technology. To realize the full potential of the NHII, supportive changes in the social, economic, and legal infrastructures are also required. Policies promoting the portability and continuity of personal health information are essential. Values, practices, relationships, laws, and investment and reimbursement policies must support the creation and use of data and information systems that are consistent with the vision for the NHII (see Chapter 3 for an additional discussion and recommendation).
COLLABORATION WITH GOVERNMENTAL PUBLIC HEALTH AGENCIES
The activities and interests of the health care delivery system and the governmental public health agencies clearly overlap in certain areas, but there is relatively little collaboration between them. In addition, the authority of state health departments in quality monitoring, licensure, and rate setting can cause serious tensions between them and health care organizations. The committee discusses the extent of this separation and the particular need for better collaboration, especially in regard to assuring access to health care services, disease surveillance activities, and partnerships toward broader health promotion efforts.
The Emergence of Separate Systems
Within the public health system in the United States, collaboration between the health care sector and governmental public health agencies is
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
generally weak. This reflects the divergence and separate development of two distinct sectors following the Second World War. Lasker and colleagues observed, "[t]he dominant, highly respected medical sector focused on individual patients, emphasizing technologically sophisticated diagnosis and treatment and biological mechanisms of disease. The considerably smaller, less well-appreciated public health sector concentrated on populations, prevention, nonbiological determinants of health, and safety-net primary care" (Lasker et al., 1997:274). As disciplines and professional fields, medicine and public health evolved with minimal levels of interaction, and often without recognition of the lost opportunities to improve the health of individuals and the population. The health care and governmental public health sectors are also very unequal in terms of their resources, prestige, and influence on public policy.
The failure to collaborate characterizes not only the interactions between governmental public health agencies and the organizations and individuals involved in the financing and delivery of health care in the private sector but also financing within the federal government. Within the Department of Health and Human Services (DHHS), the Centers for Medicare and Medicaid Services (CMS) administer the two public insurance programs with little interaction or joint planning with agencies of the U.S. Public Health Service (PHS). Even the congressional authorizing committees for these activities are separate. For example, the Substance Abuse and Mental Health Services Administration, a PHS agency, administers block grants to states to augment funding for mental health and substance abuse programs, neither of which is well supported under Medicaid. Until recently, the Medicaid waiver program, administered by CMS on behalf of the Secretary of Health and Human Services, did not provide protection of reimbursement rates for clinics within the safety-net system. At the same time, the Health Resources and Services Administration, the PHS agency charged with funding federally qualified safety-net clinics for the poor, and the Indian Health Service were both seeking funds to support the increasing deficits of these clinics due to the growing number of uninsured individuals and the low rates of reimbursement for Medicaid clinics.
The operational separation of public health and health care financing programs mirrors the cultural differences that characterize medicine and public health. American fascination with technology, science, and medical interventions and a relatively poor understanding of the determinants of health (see Chapter 2) or of the workings of the governmental public health agencies also contribute to the lower status, fewer resources, and limited influence of public health. The committee views these status and resource differences as barriers to mutually respectful collaboration and to achieving the shared vision of healthy people in healthy communities. The committee also urges greater efforts on the part of the health care
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
delivery system to meet its public health responsibilities and greater efforts on the part of governmental public health agencies to reach out to health care providers and purchasers and engage them more fully in the public health system.
The Role of Governmental Public Health Agencies as Health Care Providers
Public health departments have always differed greatly in regard to the delivery of health care services, based on the availability of such services in the community and other reasons (Moos and Miller, 1981). Some provide no personal health care services at all, whereas others provide some assortment of primary health care and safety-net services. In general, however, there has been a decrease in the number of local governmental public health agencies involved in direct service provision. In a recent survey of public health agencies, primary care or direct medical care services were the least common services provided (NACCHO, 2001). Despite this, 28 percent of local public health departments report that they are the sole safety-net providers in their communities (Keane et al., 2001).
During the 1990s, Medicaid shifted from a fee-for-service program to a managed care model. This change has been a challenge to the multiple roles of public health departments as community-based primary health care providers, safety-net providers, and providers of population-based or traditional public health services. The challenge has been both financial and organizational. First, managed care plans reimburse safety-net providers less generously than fee-for-service Medicaid providers do (under Medicaid, federally qualified health centers benefited from a federal requirement for full-cost reimbursement), and they impose administrative and service restrictions that result in reduced overall rates of compensation (IOM, 2000a). In many states and localities, these changes have decreased the revenue available to public health departments and public clinics and hospitals. In many cases, funds were no longer available for population-based essential public health services or had to be diverted to the more visibly urgent need of keeping clinics and hospitals open (CDC, 1997). The result of this interplay is that many governmental public health agencies have found themselves in a strained relationship with managed care organizations: on the one hand, encouraging their active partnership in an intersectoral public health system and, on the other, competing with them for revenues (Lumpkin et al., 1998). Second, the shift of Medicaid services to a managed care environment led some public health departments to scale down or dismantle their infrastructure for the delivery of direct medical care. The recent trend of the exit of managed care from the Medicaid market has left some people without a medical home and, in cases of
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
changes in eligibility, has left some people uninsured. This problem may be most acute in rural areas, where public health departments are often the sole safety-net providers (Johnson and Morris, 1998).
One strategy to help lessen the negative impacts of changes in health care financing undertaken by some public health departments has been the development of formal relationships (e.g., negotiating and implementing memoranda of agreement) with local managed care organizations that provide Medicaid and, in some cases, safety-net services. Such arrangements have made possible some level of integration of health care and public health services, enhanced information exchange and continuity of care, and allowed public health departments to be reimbursed for the provision of some of the services that are covered by the benefits packages of managed care plans (Martinez and Closter, 1998). At this time, governmental public health agencies are still called on to play a role in assurance broader than that which may be compatible with their other responsibilities to population health. However, closer integration between these governmental public health agencies and the health care delivery system can help address the needs of the uninsured and underinsured. Denver Health, in Colorado, provides an intriguing example of a hybrid, integrated public–private health system (Mays et al., 2000). Denver Health is the local (county and city) public health authority, as well as a managed care organization and hospital service. Although changes in the Medicaid program continue to challenge Denver Health, it continues to balance its broad responsibilities to the public's health with its role and capacity as a large health care provider.
Disease Surveillance and Reporting
Disease surveillance and reporting provide a classic exemplar of essential collaboration between the health care system and the governmental public health agencies. The latter rely on health care providers and laboratories to supply the data that are the basis for disease surveillance. For instance, in the fall of 2001, reports from physicians who diagnosed the first cases of anthrax were essential in recognizing and responding to the bioterrorism attack.
States mandate the reporting of various infectious diseases (e.g., AIDS, hepatitis B, measles, rabies, and tuberculosis) and submit data to federal disease surveillance systems (CDC, 1999). Governmental public health agencies also depend on astute clinicians to inform them of sentinel cases of recognized diseases that represent a special threat to the public's health and of unusual cases, sometimes without a confirmed diagnosis, that may represent a newly emerging infection, such as Legionnaires' disease or West Nile virus in North America. Other types of public health surveillance activities,
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
such as registries for cancer cases and for childhood immunizations, also depend on reporting from the health care system.
Effective surveillance requires timely, accurate, and complete reports from health care providers. In the case of infectious diseases, if all systems work effectively, the necessary information regarding the diagnosis for a patient with a reportable disease is transmitted to the state or local public health department by a physician or laboratory. For unusual or particularly serious conditions, public health officials offer guidance on treatment options and control measures and monitor the community for any additional reports of similar illness. For diseases like tuberculosis and sexually transmitted diseases, public health agencies facilitate active tracking and prophylactic treatment of persons exposed to an infected individual. Disease reporting requirements vary from state to state, although most states include diseases identified by the Centers for Disease Control and Prevention (CDC) as part of the National Notifiable Disease Reporting System.
Disease reporting is not complete, however. For diseases under national surveillance, from 6 to 90 percent of cases are reported, depending on the disease (Teutsch and Churchill, 1994; Thacker and Stroup, 1994). Incomplete reporting may reflect a lack of understanding by some health care providers of the role of the governmental public health agencies in infectious disease monitoring and control. In some instances, physicians and laboratories may be unaware of the requirement to report the occurrence of a notifiable disease or may underestimate the importance of such a requirement. The difficulty of reporting in a busy practice is also a barrier.
Notifiable disease reporting systems within public health departments with strong liaisons with the health care community are important in the detection and recognition of bioterrorism events. However, this valuable tool has not been well supported and, as noted earlier, suffers from issues of lack of timeliness and incomplete reporting, as well as complex or unclear reporting procedures and limited feedback from governmental public health agencies on how data are used (Baxter et al., 2000; Stagg Elliott, 2002). Health care delivery systems may fear that the data will be used to measure performance, and concerns about patient confidentiality can also contribute to a reluctance to report some diagnoses. New federal regulations regarding the confidentiality of medical records, required by the Health Insurance Portability and Accountability Act (P.L. 104–191) have generated enormous uncertainty and apprehension among health care providers and health systems regarding the sharing of individual clinical data.
Health care providers may also reduce their use of laboratory tests to confirm a diagnosis. This may be because of cost concerns or insurance plan restrictions or simply professional judgment that the test is unnecessary for appropriate clinical care. However, when fewer diagnostic tests are
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
performed for self-limiting illnesses like diarrhea, there may be delays in recognizing a disease outbreak. Reduced use of laboratory testing prevents the analyses of pathogenic isolates needed for disease tracking, testing of new pathogens, and determining the levels of susceptibility to antimicrobial agents.
Other changes in the health care delivery system also raise concerns about the infectious disease surveillance system. As patterns of health care delivery change, old reporting systems are undermined, but the opportunities offered by new types of care systems and technologies have not been realized. For example, traditional patterns of reporting may be lost as health care delivery shifts from inpatient to outpatient settings. Hospital-based epidemiological reporting systems no longer capture many diagnoses now made and treated on an outpatient basis. This would not be a problem if health care systems used currently available information technologies, including electronic medical records and internal disease surveillance systems.
Better information systems that allow the rapid and continuous exchange of clinical information among health care providers and with public health agencies have the potential to improve disease surveillance as well as aid in clinical decision making while avoiding the use of unnecessary diagnostic tests. With such a system, a physician seeing an influx of patients with severe sore throats could use information on the current community prevalence of confirmed streptococcal pharyngitis and the antibiotic sensitivities of the cultured organisms to choose appropriate medications. From a public health perspective, such a system would permit continuous analysis of data from a number of clinical sites, enabling rapid recognition and response to new disease patterns in the community (see Chapter 3 for a discussion of syndrome surveillance). For example, toxic or infectious exposures could be tracked more easily if the characteristics of every patient encounter were integrated into one system and if everyone had unimpeded access to systems of care that could generate such data.
A CDC-funded project of the Massachusetts Department of Public Health and the Harvard Vanguard Medical Associates (a large multi-specialty group) offers a glimpse of the benefits to be gained through collaboration between health care delivery systems and governmental public health agencies and specifically through the effective use of medical information systems (Lazarus et al., 2002). The Harvard Vanguard electronic medical system is queried each night for specific diagnoses assigned during the preceding day in the course of routine care. Diagnoses of interest are grouped into syndromes, and rates of new episodes are computed for all of eastern Massachusetts and each census tract. Expected numbers of new episodes are obtained from a generalized linear mixed model that uses data from 1996 to 1999. These expected numbers allow estimates of the probability of observing specific numbers of cases, either overall or in specific
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
census tracts, and the rapid identification of an unusual cluster of events. The value of this type of real-time monitoring of unusual disease outbreaks is obvious for early identification of bioterrorism attacks as well as for improvements in clinical care and population health.
Sentinel Surveillance
Reports of sentinel events have proved useful for the monitoring of many diseases, but such reports may be serendipitous and generated because of close clustering, unusual morbidity and mortality, novel clinical features, or the chance availability of medical expertise. Sentinel networks that specifically link groups of participating health care providers or health care delivery systems to a central data-receiving and -processing center have been particularly helpful in monitoring specific infections or designated classes of infections. Examples of such networks are the National Nosocomial Infections Surveillance system and the National Molecular Subtyping Network for Foodborne Disease Surveillance (PulseNet). More recently, CDC has implemented a strategy directed to the identification of emerging infectious diseases in collaboration with many public health partners. The Emerging Infections Program (EIP) is a collaboration among CDC, state public health departments, and other public health partners for the purpose of conducting population-based surveillance and research on infectious diseases. At present, nine states (California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New York, Oregon, and Tennessee) act as a national resource for the surveillance, prevention, and control of emerging infectious diseases (CDC, 2002). The EIP sites have performed investigations of meningococcal and streptococcal diseases and have established surveillance for unexplained deaths and severe illnesses as an attempt to identify diseases and infectious agents, known and unknown, that can lead to severe illness or death (CDC, 2002).
Preparing Health Care Professionals
Academic health centers (AHCs) serve as a critical interface with governmental public health agencies in several ways. First, as noted earlier, AHCs are an important part of the safety-net system in most urban areas. Second, they are the principal providers of specialized services and serve as regional referral centers for smaller towns or cities and rural areas. Both in normal periods and especially when confronted with either natural disasters or terrorist events, the specialized care units are an essential resource for public health. Moreover, they are also primary loci for research and training. AHCs also have a unique and special set of values that they bring to health care that transcend the discrete functions they perform.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
The environment in which AHCs operate has changed substantially over the past decade. The advent of managed care plans that seek services from the lowest-cost appropriate provider and changes in federal (Medicare) reimbursement policies that reduced subsidies for costs associated with AHCs' missions in education, research, and patient care have created considerable pressure on academic institutions to increase efficiency and control costs. At the same time, advances in information technology and the explosion of knowledge from biomedical research have enormous implications for the role of AHCs in the health care system and in population health. Scientific and technological advances will permit clinical care to intervene early in a disease process by identifying and modifying personal risk. The burgeoning knowledge base will require different educational approaches to use the continuously expanding evidence base, with an emphasis on continuing education and lifetime learning.
These changes may result in a broader mission for AHCs that explicitly includes improving the public's health, generating and disseminating knowledge, advancing e-health approaches (i.e., that utilize the Internet and electronic communication technologies), providing education to current health professionals, providing community service and outreach, and delivering care that has the attributes necessary for practice. The ability of academic medicine to evolve into a broader mission will depend on changes in payment systems that may be difficult to achieve and on internal changes within AHCs that may be equally difficult.
Governmental public health agencies may also play an important role in preventive medicine and public health education. Health departments, for example, provide unique venues for the training of nurses, physicians, and other health care professionals in the basics of community-based health care and gain an understanding of population-level approaches to health improvement. Furthermore, public health students and preventive medicine residents gain practical experience in health department rotations, where they participate in program planning and evaluation and learn about assessing a community's health care needs and implementing strategies that change the conditions for health.
COLLABORATION WITH OTHER PUBLIC HEALTH SYSTEM ACTORS
In addition to the linkages between the health care delivery system and governmental public health agencies, health care providers also interface with other actors in the public health system, such as communities, the media, and businesses and employers.
Relationships between the health care sector—hospitals, community health centers, and other health care providers—and the community are not
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
new and have gained increased recognition for the value they bring to health care operations, their potential for enhancing provider accountability (VHA and HRET, 2000), the knowledge and empowerment they help to create in communities, and their potential for promoting health.
The recent trend among universities to assess their level of involvement in their communities and to develop programs focused on "service learning," and such public service oriented academic work includes AHCs. Calleson and colleagues (2002) surveyed the executives and staff of eight AHCs around the country and found that community–campus partnerships can strengthen the traditional mission of AHCs. The involvement of AHCs in the communities is also likely to increase in the coming years. The AHCs surveyed listed several factors that facilitated the development of relationships with communities and community organizations, including the request of the communities themselves and the growing population health orientation of the health care sector. Furthermore, non-academic community health centers also frequently have close ties to their communities, collaborating to assess local health needs, providing needed services, and supporting community efforts with research expertise and technical assistance in planning and evaluation. Many hospitals participate in broad community-based efforts to achieve some of the conditions necessary for health, for instance, collaborating with community development corporations to contribute financial, human, and technical resources (U.S. Department of Housing and Urban Development, 2002). Montefiore Medical Center in the Bronx, New York, for example, has partnered with a local nonprofit organization to develop low- and moderate-income housing and to establish a neighborhood kindergarten (Seedco and N-PAC, 2002). Additionally, Montefiore Medical Center partners with local high schools to develop health care professions education programs intended to create new career options and improve the likelihood inner-city youth will stay in school (Montefiore Medical Center, 2001). Hospitals are also employers, and in the case of two Lawndale, Illinois, hospitals, collaboration with the local development corporation and other neighborhood organizations in 1999 made affordable local housing available to employees, helping to facilitate community development (University of Illinois, 1999). In Providence, Rhode Island, a community partnership of nonprofit and independent hospitals and colleges works to improve children's quality of life by providing school-based health services, innovative and enhanced education through teacher and staff training, and support to improve home environments through housing advocacy (Health & Education Leadership for Providence, 2001; Providence Public School District, 2002).
Many hospitals and health care systems have seen the value of going beyond the needs of the individuals who enter the health care system to engage in broader community health action, even within the constraints of
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
the current environment. The National Community Care Network Demonstration Program, sponsored by the Hospital Research and Education Trust (HRET), reports on hospitals across the country that are supporting activities beyond the delivery of medical care to improve health status and quality of life in local communities. Some of the motivation comes from the increasing pressure on nonprofit hospitals to justify their tax-exempt status through the provision of services that benefit the community, largely the provision of charity care; yet, many are seeing that investments in community health improvement are greater in value than the provision of medical care for preventable diseases (Barnett and Torres, 2001).
Vignettes drawn from the experience of American Hospital Association NOVA Award recipients illustrate the importance of investing in overall community health (AHA, 2002). For example, in 1994, Parkland Health and Hospital System in Dallas noted that injury rates in the community were three times the national average and that trauma admissions had jumped 38 percent in one year (53 percent of that care is uncompensated). As a result, the organization decided to convene the county's leading trauma care providers, police, and civic groups to investigate and solve the problem. With start-up funding from a local foundation, its own fundraising, and annual corporate sponsorships ranging from $35,000 to $150,000 from local hospitals and businesses, the coalition launched a Safe Communities initiative with a 52-member community advisory panel. Coalition members decided to tackle, in order, injuries caused by car accidents, violence, falls, and burns, through 11 initiatives involving more than 80 community organizations and agencies. Over a 2-week period, there was a 13 percent reduction in trauma admissions from car crashes due to a public awareness campaign and police initiative (AHA, 2002).
A 1998 finalist for the Foster G. McGaw Prize for Excellence in Community Service co-sponsored by AHA, the Franklin Community Health Network (FCHN) in Farmington, Maine, took the lead in developing a coalition and providing seed money to start a Rural Schools Equity Campaign (AHA, 2002). With high levels of youth involvement, and media cooperation, the campaign led to the legislative reformulation of property taxes to increase funding for rural schools in FCHN's service area by $1.3 million. In a further example, the Crozer-Keystone Health System that serves Chester, Pennsylvania, was declared a distressed municipality by the state in 1994. Although at the time the health system had been increasing its health care outreach programs, it realized it had to look at "root causes." As the largest employer in Chester, the system organized Community Connections, a mosaic of health, economic, and social programs and services developed in partnership with 20 other organizations, a local university, and governmental agencies. Programs included attracting other businesses to Chester, setting up a business incubator building, and colocating multiple health and
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
social programs to facilitate "one-stop shopping." The effort has had a major stabilizing effect on Chester, and although overall health indicators are still behind state averages for chronic diseases, they are improving. Immunization rates have improved from 36 to 99 percent, and teen pregnancy is down to 31 per 1,000 from 44 per 1,000.
Under the guidance of an external review panel, HRET and the Voluntary Hospital Association of America (VHA) Health Foundation reviewed the experiences of recipients of the Foster G. McGaw Prize3 from 1986 to 1998 and VHA Community Health Improvement Leadership Awards from 1996 to 1998. Fifteen of 20 winners participated in a study, which included a self-assessment of changes since the time of the award and in-depth interviews with chief executive officers, trustees, and those leading the initiative. Although this survey serves only as an illustration of what may be possible, several elements appeared supportive of a sustained commitment to efforts at community health improvement. These included
-
Committing leadership at multiple levels through the top leadership to sustain changes;
-
Developing community partnerships to develop champions outside the organization;
-
Protecting funding and leadership of community health initiatives while integrating community health values into the culture of the parent organization;
-
Linking community work with clinical work (mission alignment);
-
Building an evidence base through evaluation and ongoing measurement of community health indicators; and
-
Exploring external revenue streams and advocating for changes in current health care financing and funding for such efforts (VHA Health Foundation and HRET, 2000).
Boufford (1999) has suggested a Community Health Improvement Strategy that identifies a number of steps that provider organizations can take in such community-based efforts (see Box 5–9). However, payment systems are critical to encourage and sustain these network initiatives, and current reimbursement policies in public and private insurance are not designed to support population-focused care in a noncapitated system.
The health care sector can also develop linkages with the media to help ensure the accuracy of health information, communicate risk, and facilitate the public understanding of health care. For example, health care organiza
| 3 | The Foster G. McGaw Prize for Excellence in Community Service is awarded by the American Hospital Association to recognize hospitals that have distinguished themselves through efforts to improve the health and well-being of everyone in their communities. |
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
BOX 5–9 Community Health Improvement Strategy
-
Identify a defined population ("community") and develop links to that community
-
Assess health status and need, and adjust the volume and types of services provided to respond to the health needs of the community
-
Develop effective primary care systems
-
Develop effective intervention programs in partnership with the community
-
Address the health status of the institutional workforce
-
Develop staff as an effective force for community health
-
Serve as an advocate in the community to increase healthy choices available to the population
-
Use economic leverage within the community for "health-related" changes
-
Jobs for community residents
-
Channeling purchasing power into community business
-
Housing development through capital leverage
SOURCE: Boufford (1999:291).
tions may use the media to disseminate health care information to their market areas, as demonstrated by the Minneapolis Allina Health System in its collaboration with a local television station and a health care news provider (Rees, 1999). Additionally, the media may be a powerful tool for familiarizing the public with health and health care issues and a conduit for raising important questions, stimulating public interest, or even influencing the public's health behaviors. For example, the popular prime time television show ER frequently serves as a platform for health information, with episodes exploring topics such as childhood immunizations, contraception, and violence (Brodie et al., 2001; also see Chapter 7).
Businesses and employers most commonly interface with the health care sector in purchasing and designing employee health benefits, with goals such as the inclusion of comprehensive preventive health care services. However, there are examples of wide-reaching business–health care linkages, such as the efforts to ensure quality of care and enhanced consumer choice undertaken by the Pacific Business Group on Health (see Chapter 6). Chapter 4 provides additional examples of fruitful community partnerships involving the health care sector.
IMPLICATIONS OF GROWING HEALTH CARE COSTS
As the committee has noted, health-related (mostly health care-related) spending in the United States amounted to $1.3 trillion in 2000, about 13.2
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
percent of the gross domestic product (Levit et al., 2002). After a period of stability in the mid-1990s, health care costs are again rising because of several factors (Heffler et al., 2002). Prescription drug spending, in particular, has increased sharply, and increased by 17.3 percent from 1999 to 2000 (HCFA, 2002). This increase comes from the growth of the older population and the proportion of the overall population with chronic conditions, along with the introduction of new and more expensive drugs, many of which are used to treat chronic conditions. In addition, spending for hospital services increased by 5.1 percent between 1999 and 2000, reaching $412 billion, and the cost of nursing home and home health care increased by 3.3 percent (Levit et al., 2002). However, the increase in health spending also reflects the success of federal and state efforts to enroll more low-income children in Medicaid and the State Children's Health Insurance Program, increased enrollment in Medicare as the population ages, and some erosion of unpopular cost-control features imposed by managed care plans.
With the economic downturn in 2001, the growth in health care spending creates added financial burdens for everyone, including individuals seeking care or insurance coverage, employers offering health insurance benefits, and governments at the federal, state, and local levels managing publicly funded insurance programs (Fronstin, 2002; Trude et al., 2002). Substantial increases in health insurance premiums are a clear indication of these economic stresses. For example, the California Public Employees' Retirement System, which is the nation's second largest public purchaser of employee health benefits, recently announced that health insurance premiums would increase by 25 percent (Connoly, 2002). States are experiencing serious pressures from growth in Medicaid spending, which increased by about 13 percent from 2001 to 2002, following a 10.6 percent increase in 2001 (NASBO, 2002a). With revenues increasing by only about 5 percent in the same period, Medicaid now accounts for more than 20 percent of total state spending (NASBO, 2002b).
The growing cost of health care has obvious implications for the nation's readiness to address the problems discussed in this chapter. Providing coverage to the uninsured, improving coverage for certain types of care, strengthening the emergency response and surge capacity in the hospital sector, and investing in information systems that can improve the quality of individual care and population-based disease surveillance will all require significant new resources from the public and private sectors. Although these steps can be expected to improve the nation's health and may even reduce costs over time, the initial investment will be substantial. The committee is concerned that with the escalation of expenditures, going in large measure toward maintaining current services, it will be difficult to identify
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
the necessary public- and private-sector resources that will be needed for new activities.
The committee recommends that bold, large-scale demonstrations be funded by the federal government and other major investors in health care to test radical new approaches to increase the efficiency and effectiveness of health care financing and delivery systems. The experiments should effectively link delivery systems with other components of the public health system and focus on improving population health while eliminating disparities. The demonstrations should be supported by adequate resources to enable innovative ideas to be fairly tested.
CONCLUDING OBSERVATIONS
This chapter has outlined the main areas in which the health care delivery system and the governmental public health agencies interface. These areas include the regulatory and quality monitoring functions performed by governmental agencies, disease surveillance and reporting by health care providers, and the provision of safety-net services. Although assurance is a core function of public health, governmental public health agencies often do more than assure that people can access health care services; public health departments may become providers of last resort in areas where no other services are available for low-income, uninsured populations and when managed care services to Medicaid and uninsured populations are discontinued. These circumstances force public health departments to provide personal health care services instead of using their resources and population-level approaches to guide and support community efforts to change the conditions for health. Closer collaboration and integration between governmental public health agencies and the health care delivery system may enhance the capacities of both to improve population health and may support the efforts of other public health system actors.
REFERENCES
AAMC (Association of American Medical Colleges). 2000. Minority Graduates of US Medical Schools: Trends, 1950–1998. Washington, DC: Association of American Medical Colleges.
AHA (American Hospital Association). 2001a. Emergency departments—an essential access point to care. AHA TrendWatch 3(1).
AHA. 2001b. The health care workforce shortage and its implication for America's hospitals. AHA Workforce Survey Results. Available online at www.aha.org/workforce/resources. Accessed April 9, 2002.
AHA. 2002. Nova Award Winners 1994–200. Available online at www.hospitalconnect.com/aha/awards-events/awards/novaaward.html. Accessed October 7, 2002.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
AHCPR (Agency for Health Care Policy and Research). 1993. Depression in Primary Care: Treatment of Major Depression. Rockville, MD: Department of Health and Human Services.
Aiken L, Clarke S, Sloane D, Sochalski J, Busse R, Clarke H, Giovannetti P, Hunt J, Rafferty A, Shamian J. 2001. Nurses' report on hospital care in five countries. Health Affairs 20(3):43–53.
Aiken LH, Smith HL, Lake ET. 1994. Lower Medicare mortality among a set of hospitals known for good nursing care. Medical Care 32:771–787.
Allukian M. 1999. Dental insurance is essential, but not enough. In Closing the Gap, a newsletter. July. Washington, DC: Office of Minority Health, Department of Health and Human Services.
American Medical Association. 1998. Socioeconomic characteristics of medical practice 1997/ 98. Chicago: American Medical Association.
Andrulis DP, Kellermann A, Hintz EA, Hackman BB, Weslowski VB. 1991. Emergency departments and crowding in United States teaching hospitals. Annals of Emergency Medicine 20(9):980–986.
Ayanian JZ, Weissman JS, Schneider EC, Ginsburg JA, Zaslavsky AM. 2000. Unmet health needs of uninsured adults in the United States. Journal of the American Medical Association 284:2061–2069.
Bajuscak R. 1999. Warning signs in the mouth. In Closing the Gap, a newsletter. July. Washington, DC: Office of Minority Health, Department of Health and Human Services.
Baker DW, Shapiro MF, Schur CL. 2000. Health insurance and access to care for symptomatic conditions. Archives of Internal Medicine 160(9):1269–1274.
Barnett K, Torres G. 2001. Beyond the Medical Model: Hospitals Improve Community Building. Community Care Network (CCN) Briefings, Fall 2001. Chicago, IL: Hospital Research and Education Trust, American Hospital Association.
Bates D, Cohen M, Leape LL, Overhage JM, Shabot MM, Seridan T. 2001. Reducing the frequency of errors in medicine using information technology. Journal of the American Medical Informatics Association 8(4):299–308.
Bates DW, Leape LL, Culled DJ, Laird N, Petersen LA, Teito JM, Burdick E, Hickey M, Kleefield S, Shea B, Vander Vliet M, Seger DL. 1998. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. Journal of the American Medical Association 280(15):1311–1316.
Baxter R, Mechanic RE. 1997. The status of local health care safety-nets. Health Affairs 16(4):7– 23.
Baxter R, Rubin R, Steinberg C, Carroll C, Shapiro J, Yang A. 2000. Assessing Core Capacity for Infectious Diseases Surveillance. Final Report prepared for the Office of the Assistant Secretary for Planning and Evaluation. Falls Church, VA: The Lewin Group, Inc.
Berk ML, Schur C. 1998. Access to care: how much difference does Medicaid make? Health Affairs 17:169–108.
Billings J, Zeitel L, Lukomnik J, Carey TS, Blank AE, Newman L. 1993. Impact of socioeconomic status on hospital use in New York City. Health Affairs 12(1):162–173.
Billings J, Anderson G, Newman L. 1996. Recent findings on preventable hospitalizations. Health Affairs 15(3):239–249.
Bindman AB, Grumbach K, Osmond D, Komaromy M, Vranizan K, Lurie N, Billings J, Stewart A. 1995. Preventable hospitalizations and access to health care. Journal of the American Medical Association 274:305–311.
Blendon RJ, Scoles K, DesRoches C, Young JT, Herrmann MJ, Schmidt JL, Kim M. 2001. Americans' health priorities: curing cancer and controlling costs. Health Affairs 20(6):222– 232.
Bloche MG. 2001. Race and discretion in American medicine. Yale Journal of Health Policy, Law and Ethics 1:95–131.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Boards of Trustees, Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. 2002. 2002 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Available online at http://cms.hhs.gov/publications/trusteesreport/default.asp. Accessed October 6, 2002.
Boufford JI. 1999. Health future: the managerial agenda. Journal of Health Administration Education 17(4):271–295.
Breen N, Wagener DK, Brown ML, Davis WW, Ballard-Barbash R. 2001. Progress in cancer screening over a decade: results of cancer screening from the 1987, 1992, and 1998 National Health Interview Surveys. Journal of the National Cancer Institute 93:1704–1713.
Brewster LR, Rudell LS, Lesser CS. 2001. Emergency room diversions: a symptom of hospitals under stress . Issue Brief No. 38. Washington, DC: Center for Studying Health System Change.
Brodie M, Foehr U, Rideout V, Baer N, Miller C, Flournoy R, Altman D. 2001. Communicating health information through the entertainment media: a study of the television drama ER lends support to the notion that Americans pick up information while being entertained. Health Affairs 20(1):192–199.
Burstin HR, Swartz K, O'Neill AC, Orav EJ, Brennan TA. 1998. The effect of change of health insurance on access to care. Inquiry 35:389–397.
Calleson DC, Seifer SD, Maurana C. 2002. Forces affecting community involvement of AHCs: perspectives of institutional and faculty leaders. Academic Medicine 77(1):72–81.
CDC (Centers for Disease Control and Prevention). 1997. Estimated expenditures for essential public health services-selected states, fiscal year 1995. Morbidity and Mortality Weekly Report 46(7):150–152.
CDC. 1998. Use of clinical preventive services by adults aged <65 years enrolled in health-maintenance organizations—United States, 1996. Morbidity and Mortality Weekly Report 47(29):613–619.
CDC. 1999. Summary of notifiable diseases, United States, 1999. Morbidity and Mortality Weekly Report 48(53):1–104.
CDC. 2002. Emerging Infections Program. CDC, National Center for Infectious Diseases Surveillance Resources. Available online at www.cdc.gov/ncidod/osr/EIP.htm. Accessed October 21, 2002.
CMS (Centers for Medicare and Medicaid Services). 2002a. CMS program operations. Section II. In Program Information on Medicare Medicaid, SCHIP & Other Programs of the Centers for Medicare & Medicaid Services. Available online at http://cms.hhs.gov/charts/series/. Accessed October 4, 2002.
CMS. 2002b. Medicare program information, Section III.B.1. In Program Information on Medicare Medicaid, SCHIP & Other Programs of the Centers for Medicare & Medicaid Services. Available online at http://cms.hhs.gov/charts/series/. Accessed October 4, 2002.
CMS. 2002c. State Children's Health Insurance Program: Fiscal year 2001 annual enrollment report. Available online at www.cms.hhs.gov/schip/schip01.pdf. Accessed October 15, 2002.
Coffey RM, Mark T, King E, Harwood H, McKusick D, Genuardi J, Dilonardo J, Chalk M. 2001. National Estimates of Expenditures for Substance Abuse Treatment, 1997. Rockville, MD: Center for Substance Abuse Treatment, Substance Abuse and Mental Health Services Administration, Department of Health and Human Services.
Connolly C. 2002. Health-care costs jump at CalPERS: big premium increase may signal trend. Washington Post, April 17, p. E01.
Cooper-Patrick L, Gallo JJ, Powe NR, Steinwachs DM, Eaton WW, Ford DE. 1999. Mental health service utilization by African Americans and whites: The Baltimore Epidemiologic Catchment Area Follow-up. Medical Care 37:1034–1045.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Department of Defense. 2002. TRICARE Homepage. Available online at www.tricare.osd.mil. Accessed August 3, 2002.
Department of Veterans Affairs. 1993. Clinical Guidelines for Major Depressive Disorder. Washington, DC: Veterans Health Administration.
Derlet R, Richards J, Kravitz R. 2001. Frequent overcrowding in U.S. emergency departments. Academic Emergency Medicine 8(2):151–155.
DHHS (Department of Health and Human Services). 1999. Mental Health: A Report of the Surgeon General. Rockville, MD: Substance Abuse and Mental Health Administration, National Institute of Mental Health, National Institutes of Health, Department of Health and Human Services.
DHHS. 2000a. Objective 18: mental health and mental disorders. In Healthy People 2010, Vol. II, 2nd ed.Washington, DC: Department of Health and Human Services.
DHHS. 2000b. Oral Health in America: A Report of the Surgeon General. Rockville, MD: National Institute of Dental and Craniofacial Research, National Institutes of Health, Department of Health and Human Services.
DHHS. 2002. 2002 CMS Statistics. CMS Publication 03437. Baltimore, MD: Department of Health and Human Services. Available online at http://cms.hhs.gov/researchers/pubs/CMSStatisticsBlueBook2002.pdf. Accessed online October 15, 2002.
Dranove D, Simon CJ, White WD. 2002. Is managed care leading to consolidation in healthcare markets? Health Services Research 37(3):573–594.
Draper DA, Hurley RE, Lesser CC, Strunk BC. 2002. The changing face of managed care. Health Affairs 21(1):11–23.
Farley T, Flannery JT. 1989. Late-stage diagnosis of breast cancer in women of lower socioeconomic status: public health implications. American Journal of Public Health 79:1508– 1512.
Franks P, Fiscella K. 1998. Primary care physicians and specialists as personal physicians. Health care expenditures and mortality experience. Journal of Family Practice 47:105– 109.
Fronstin D. 2002. Trends in health insurance coverage: a look at early 2001 data. Health Affairs 21(1):188–193.
GAO (General Accounting Office). 2000. Oral health: dental disease is a chronic problem among low-income populations. Letter Report GAO/HEHS-00-72, April 12. Washington, DC: General Accounting Office.
GAO. 2001a. Medicaid: Stronger Efforts Needed to Ensure Children's Access to Health Screening Services. Report to Congressional Requesters, GAO-01-749. Washington, DC: General Accounting Office.
GAO. 2001b. Strategic objective: the health needs of an aging and diverse population. In Strategic Plan 2002–2007. Available online at www.gao.gov. Accessed October 6, 2002.
Glick M. 1999. The mouth is a mirror of the body. In Closing the Gap, a newsletter. July. Washington, DC: Office of Minority Health, Department of Health and Human Services.
Haas JS, Adler NE. 2001. The causes of vulnerability: disentangling the effects of race, socioeconomic status and insurance coverage on health. Background paper prepared for the Institute of Medicine Committee on the Consequences of Uninsurance.
Hadley J, Steinberg EP, Feder J. 1991. Comparison of uninsured and privately insured hospital patients: condition on admission, resource use, and outcome. Journal of the American Medical Association 265(3):374–379.
Harris Interactive. 2001. Computing in the physician's practice. A Harris Interactive Study. Available online at www.harrisinteractive.com/. Accessed July 29, 2002.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Hayward RA, Shapiro MF, Freeman HE, Corey CR. 1988. Inequities in health services among insured Americans: do working-age adults have less access to medical care than the elderly? New England Journal of Medicine 318(23):1507–1512.
HCFA (Health Care Financing Administration). 2001. Your Medicare Benefits: Your Health Care Coverage in the Original Medicare Plan for Part A (Hospital Insurance), Part B (Medical Insurance), including Preventive Services. Publication No. HCFA – 10116. Baltimore, MD: Federal Medicare Agency, Health Care Financing Administration, Department of Health and Human Services.
HCFA. 2002. National health expenditures. Available online at www.hcfa.gov/stats/NHEOAct/. Accessed April 17, 2002.
Heffler S, Smith S, Won G, Clemens MK, Keehan S, Zezza M. 2002. Trends: health spending projections for 2001–2011: the latest outlook. Health Affairs 21(2):207–218.
HELP (Health & Education Leadership for Providence). 2001. Building the city's future: HELP's impact on the Providence economy. Prepared by Appleseed for HELP. Available online at www.helprov.org/pubs/building.pdf. Accessed October 18, 2002.
Henry J. Kaiser Family Foundation and Health Research and Educational Trust (HRET). 2000. Employer Health Benefits: 2000 Annual Survey. Primary authors: Levitt L, Holve E, Wang J, Gabel JR, Whitmore HH, Pickreign JD, Miller N, Hawkins S. Menlo Park, CA and Chicago: Henry J. Kaiser Family Foundation and HRET.
Hetzel L, Smith A. 2001. The 65 Years and Over Population: 2000. Census 2000. October. U.S. Bureau of the Census, Department of Commerce.
HRSA (Health Resources and Services Administration). 2001. The Registered Nurse Population, March 2000. Rockville, MD: Health Resources and Services Administration, Department of Health and Human Services.
Hsia J, Kemper E, Kiefe C, Zapka J, Sofaer S, Pettinger M, Bowen D, Limacher M, Lillington L, Mason E. 2000. The importance of health insurance as a determinant of cancer screening: evidence from the Women's Health Initiative. Preventive Medicine 31(3):261– 270.
IHS (Indian Health Service). 2002a. Year 2002 IHS profile. Available online at http://info.ihs.gov/Infrastructure/Infrastructure6.pdf. Accessed October 1, 2002.
IHS. 2002b. Indian Health Service 10 year expenditure trends. Available online at www.his.gov/nonmedicalprograms/ihdt2/bd/IHS10YR.pdf. Accessed August 5, 2002.
IOM (Institute of Medicine). 1996. In Wunderlich GS, Sloan FA, Davis CK (Eds.). Nurse Staffing in Hospitals and Nursing Homes: Is It Adequate? Washington, DC: National Academy Press.
IOM. 1998. In Edmunds M, Coye MJ (Eds.). America's Children: Health Insurance and Access to Care. Committee on Children, Health Insurance, and Access to Care, Institute of Medicine and National Research Council. Washington, DC: National Academy Press.
IOM. 2000a. America's Health Care Safety Net: Intact but Endangered. Washington, DC: National Academy Press.
IOM. 2000b. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press.
IOM. 2001a. Coverage Matters: Insurance and Health Care. Washington, DC: National Academy Press.
IOM. 2001b. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press.
IOM. 2001c. The Right Thing to Do, The Smart Thing to Do: Enhancing Diversity in Health Professions. Summary of the Symposium on Diversity in Health Professions in Honor of Herbert W. Nickens, M.D. Washington, DC: National Academy Press.
IOM. 2002a. Care Without Coverage: Too Little, Too Late. Washington, DC: The National Academies Press.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
IOM. 2002b. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health. Washington, DC: The National Academies Press.
IOM. 2002c. Setting the Course: A Strategic Vision for Immunization Part 1: Summary of the Chicago Workshop . Committee on the Immunization Finance Dissemination Workshops, Division of Health Care Services, Institute of Medicine. Washington, DC: The National Academies Press.
Johnson R, Morris TF (Ed.). 1998. Stabilizing the Rural Health Infrastructure. National Advisory Committee on Rural Health. Health Resources and Services Administration and the North Carolina Rural Health Research and Policy Analysis Program, the Cecil G. Sheps Center for Health Services Research, University of North Carolina at Chapel Hill.
Jones R, McConville J, Mason D, Macpherson L, Naven L, McEwen J. 1999. Attitudes towards, and utility of, an integrated medical-dental patient-held record in primary care. British Journal of General Practice 49(442):368–373.
Kaiser Family Foundation and Health Research and Educational Trust. 2000. 2000 Employer Health Benefits Survey. Menlo Park, CA: The Henry J. Kaiser Family Foundation.
Kasper JD, Giovannini TA, Hoffman C. 2000. Gaining and losing health insurance: strengthening the evidence for effects on access to care and health outcomes. Medical Care Research and Review 57(3):298–318.
Keane C, Marx J, Ricci E. 2001. Local health departments' changing role in provision and assurance of safety-net services. A project funded by the Center for Health Services Financing and Managed Care of the Health Resources and Service Administrative through a cooperative agreement with the Association of Schools of Public Health.
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. 1994. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Archives of General Psychiatry 51:8–19.
King JS. 2000. Grant results report: assessing insurance coverage of preventive services by private employers. Robert Wood Johnson Foundation. Available online at www.rwjf.org/app/rw_grant_results_reports/rw_grr/029975s.htm. Accessed April 19, 2002.
Krall MA. 1998. Achieving clinician use and acceptance of the electronic medical record. The Permanente Journal 2(10):48–53.
Lasker RD, Committee on Medicine and Public Health. 1997. Medicine and Public Health: The Power of Collaboration. New York: The New York Academy of Medicine.
Lazarus R, Kleinman K, Dashevsky I, Adams C, Kludt P, DeMaria A Jr, Platt R. 2002. Use of automated ambulatory-care encounter records for detection of acute illness clusters, including potential bioterrorism events. Emerging Infectious Diseases 8(8):753–760.
Legnini MW, Anthony SE, Wicks EK, Mayer JA, Rybowski LS, Stepnick LS. 1999. Summary of Findings: Privatization of Public Hospitals. Prepared for the Henry J. Kaiser Family Foundation by the Economic and Social Research Institute. Available online at: www.kff.org/content/archive/1450/private_s.pdf. Accessed September 2, 2002.
Leigh WA, Lillie-Blanton M, Martinez RM, Collins KS. 1999. Managed care in three states: experiences of low-income African Americans and Hispanics. Inquiry 36:318–331.
Levit K, Smith C, Cowan C, Lazenby H, Martin A. 2002. Inflation spurs health spending in 2000. Health Affairs 21(1):172–181.
Lumpkin JR, Landrum LB, Oldfield A, Kimel P, Jones MC, Moody CM, and Turnock BJ. 1998. Impact of Medicaid resources on core public health responsibilities of local health departments in Illinois. Journal of Public Health Management and Practice 4(6):69–78.
Lurie N, Ward NB, Shapiro MF, Brook RH. 1984. Termination from Medi-Cal: does it affect health? New England Journal of Medicine 311:480–484.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Lurie N, Ward NB, Shapiro MF, Gallego C, Vaghaiwalla R, Brook RH. 1986. Termination of Medi-Cal benefits: a follow-up study one year later. New England Journal of Medicine 314:1266–1268.
Macinko JA, Starfield B, Shi L. [in press]. The Contribution of Primary Care Systems to Health Outcomes within Organization for Economic Cooperation and Development (OECD) Countries, 1970–1998. Health Services Research.
Mandelblatt J, Andrews H, Kerner J, Zauber A, Burnett W. 1991. Determinants of late stage diagnosis of breast and cervical cancer. American Journal of Public Health 81:646–649.
Mandelblatt J, Andrews H, Kao R, Wallace R, Kerner J. 1996. The late-stage diagnosis of colorectal cancer: demographic and socioeconomic factors. American Journal of Public Health 86:1794–1797.
Mandelblatt JS, Gold K, O'Malley AS, Taylor K, Cagney K, Hopkins JS, Kerner J. 1999. Breast and cervix cancer screening among multiethnic women: role of age, health and source of care. Preventive Medicine 28(4):418–425.
Mark DH, Gottlieb MS, Zellner BB, Chetty VK, Midtling JE. 1996. Medicare costs in urban areas and the supply of primary care physicians. Journal of Family Practice 43:33–39.
Markus A, Roby D, Rosenbaum S. 2002. A profile of federally funded health centers serving a higher proportion of uninsured patients. Prepared for the Kaiser Commission on Medicaid and the Uninsured. Available online at http://www.kff.org/content/2002/4033/. Accessed October 6, 2002.
Martinez RM, Closter E. 1998. Public Health Departments Adapt to Medicaid Managed Care. Issue Brief No. 16. Washington, DC: Center for Studying Health System Change.
Mays GP, Miller CA, Halverson PK. 2000. Local Public Health Practice: Trends & Models. Washington, DC: American Public Health Association.
McGinnis JM, Foege WH. 1993. Actual causes of death in the United States. Journal of the American Medical Association 270(18):2207–2212.
McManus M. 2001. Emergency department overcrowding in Massachusetts : making room in our hospitals. The Massachusetts Health Policy Forum, Issue Brief No. 12. Discussion moderated by CM McManus.
Meadows M. 1999. Making oral health a priority. In Closing the Gap, a newsletter. July. Washington, DC: Office of Minority Health, Department of Health and Human Services.
Mills RJ. 2000. Health Insurance Coverage: Consumer Income. Current Population Reports P60-211. Washington, DC: U.S. Bureau of the Census.
Mills RJ. 2002. Health Insurance Coverage: 2001. Current Population Reports, P60–220. Washington, DC: U.S. Bureau of the Census, Department of Commerce.
Mitchell JB, McCormack LA. 1997. Time trends in late-stage diagnosis of cervical cancer: differences by race/ethnicity and income. Medical Care 35(12):1220–1224.
Montefiore Medical Center. 2001. Community relations. Available online at www.montefiore.org/about/community/services/. Accessed October 21, 2002.
Moos MK, Miller CA. 1981 Relationships between public and private providers of health care. Public Health Reports 96(5):434–438.
Murray CJL, Lopez AD. 1996. The Global Burden of Disease. A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries, and Risk Factors in 1990 and Projected to 2020. Cambridge, MA: Harvard University Press.
NACCHO (National Association of County and City Health Officials). 2001. Local Public Health Agency Infrastructure: A Chartbook. Washington, DC: NACCHO.
NASBO (National Association of State Budget Officials). 2002a. Medicaid and Other Health Care Issues. 2002. Medicaid and Other State Healthcare Issues: The Current Situation. Washington, DC: NASBO and National Governors' Association.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
NASBO. 2002b. NASBO analysis: Medicaid to stress state budgets severely into fiscal 2003. Available online at www.nasbo.org/Publications/PDFs/medicaid2003.pdf. Accessed October 13, 2002.
NCHS (National Center for Health Statistics). 2002. Early release of selected estimates based on data from the January–June 2001 National Health Interview Survey. Available online at www.cdc.gov/nchs/nhis.htm. Accessed March 2, 2002.
NCVHS (National Committee on Vital and Health Statistics). 2002. Information for Health: A Strategy for Building the National Health Information Infrastructure. Report and Recommendations from the National Committee on Vital and Health Statistics. Atlanta, GA: NCVHS, CDC.
Needleman J, Buerhaus PI, Mattke S, Stewart M, Zelevinsky K. 2001. Nurse Staffing and Patient Outcomes in Hospitals. Final Report. Contract No. 230-99-0021. Washington, DC: Health Resources and Services Administration, Department of Health and Human Services.
NRC (National Research Council). 2000. Networking Health: Prescriptions for the Internet. Washington, DC: National Academy Press.
Office of the President of the United States. 2001. The budget for fiscal year 2002. Office of Management and Budget. Available online at www.whitehouse.gov/omb/budget/fy2002/bdg12.htm. Accessed June 14, 2002.
Olson K, Perkins J, Pate T. 1998. Children's Health under Medicaid: A National Review of Early Periodic Screening, Diagnosis and Treatment. Washington, DC: National Health Law Program.
O'Malley AS, Mandelblatt J, Gold K,Cagney KA, Kerner J. 2001. Continuity of care and the use of breast and cervical cancer screening services in a multiethnic community. Archives of Internal Medicine 157:1462–1470.
OPM (Office of Personnel Management). 2001. Fiscal Year 2001 performance and accountability report. Consolidated Financial Statements and Appendix A. Available online at www.opm.gov/gpra/opmgpra/par2002/. Accessed October 18, 2002.
Pacific Business Group on Health. 2002. Driving the market to reduce medical errors through the Leapfrog California Patient Safety Initiative. Available online at www.pbgh.org/programs/leapfrog/default.asp. Accessed September 27, 2002.
Partnership for Prevention. 1999. Why Invest in Disease Prevention? Results from the William M. Mercer/Partnership for Prevention Survey of Employer Sponsored Plans. Washington, DC: Partnership for Prevention.
Partnership for Prevention. 2001. Prevention Priorities: Employers' Guide to the Highest Value Preventive Health Services. Washington, DC: Partnership for Prevention.
Pew Environmental Health Commission. 2001. Transition Report to the New Administration: Strengthening Our Public Health Defense Against Environmental Threats January 17. Baltimore: Pew Environmental Health Commission.
Phillips KA, Mayer ML, Aday LA. 2000. Barriers to care among racial/ethnic groups under managed care. Health Affairs 19:65–75.
Politzer RM, Yoon J, Shi L, Hughes R, Regan J, Gaston M. 2001. Inequality in America: the contribution of health centers in reducing and eliminating disparities in access to care. Medical Care Research and Review 58:234–248.
Providence Public School District. 2002. Community partners in education. Available online at www.providenceschools.org/community_groups.cfm. Accessed September 26, 2002.
Rabinowitz J, Bromet EJ, Lavelle J, Hornak KJ, Rosen B. 2001. Changes in insurance coverage and extent of care during the two years after first hospitalization for a psychotic disorder. Psychiatric Services 52(1):87–91.
Rees T. 1999. Demand for health care information prompts media–institution alliances. Profiles in Healthcare Marketing 15(5):24–28.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Regier DA, Narrow W, Rae DS, Manderscheid RW, Locke BZ, Goodwin FK. 1993. The de facto US mental and addictive disorders service system. Epidemiologic Catchment area prospective 1-year prevalence rates of disorders and services. Archives of General Psychiatry 50:85–94.
Reinhardt UE, Hussey PS, Anderson GF. 2002. Cross-national comparisons of health systems using OECD data, 1999. Health Affairs 21(3):169–181.
Rice DP, Miller LS. 1996. The economic burden of schizophrenia: conceptual and methodological issues, and cost estimates. In Moscarelli M, Rupp A, Sartorious N (Eds.). Handbook of Mental Health Economics and Health Policy: Schizophrenia, Vol. 1. New York: John Wiley & Sons.
Rice T, Pourat N, Levan R, Silbert LJ, Brown ER, Gabel J, Kim J, Hunt KA, Hurst KM. 1998. Trends in job-based health insurance coverage. Los Angeles, CA: UCLA Center for Health Policy Research and KPMG Peat Marwick.
Robert Wood Johnson Foundation (RWJF). 2001. Substance Abuse: The Nation's Number One Health Problem. Key Indicators for Policy. February 2001 update. Waltham, MA: The Schneider Institute for Health Policy, Brandeis University.
Rosenbach ML, Gavin NI. 1998. Early and periodic screening, diagnosis and treatment and managed care. Annual Review of Public Health 19:507–525.
Schiff GD, Aggarwal HC, Kumad S, McNutt RA. 2000. Prescribing potassium despite hyperkalemia: medication errors uncovered by linking laboratory and pharmacy information systems. American Journal of Medicine 109(6):494–497.
Schoen C, DesRoches C. 2000. Uninsured and unstably insured: the importance of continuous insurance coverage. Health Services Research 35(1 Pt 2):187–206.
Schoenbaum M, Unützer J, Sherbourne C, Duan N, Rubinstein LV, Miranda J, Carney MF, Wells K. 2001. Cost-effectiveness of practice-initiated quality improvement for depression. Journal of the American Medical Association 286(11):1325–1330.
Schulberg H, Katon W, Simon G, Rush AJ. 1999. Best clinical practice: guidelines for managing major depression in primary care. Journal of Clinical Psychiatry, 60(Suppl. 7):19–24.
Seedco and the Non-Profit Assistance Corporation (N-PAC). 2002. Case studies: Montefiore Medical Center Loan. Available online at www.seedco.org/loan/case/montefiore.html. Accessed October 21, 2002.
Sherer RA. 2001. How can a nursing shortage be prevented? Geriatric Times 2(4). Available online at www.geriatrictimes.com/g010704a.html. Accessed March 2, 2002.
Shi L, Starfield B, Kennedy BP, Kawachi I. 1999. Income inequality, primary care, and health indicators. Journal of Family Practice 48:275–284.
Smith V, Ellis E, Gifford K, Ramesh R, Wachino V. 2002. Medicaid spending growth: results from a 2002 Survey. Health Management Associates and Kaiser Commission on Medicaid and the Uninsured. Available online at www.kff.org/content/2002/4064/. Accessed October 6, 2002.
Solanki G, Schauffler HH, Miller LS. 2000. The direct and indirect effects of cost-sharing on the use of preventive services. Health Services Research 34(6):1331–1350.
Solis JM, Marks G, Garcia M, Shelton D. 1990. Acculturation, access to care, and use of preventive services by Hispanics: findings from NHANES, 1982–1984. American Journal of Public Health 80(Suppl.):11–19.
Spratley E, Johnson A, Sochalski J, Fritz M, Spencer W. 2000. The Registered Nurse Population. Findings from the National Sample Survey of Registered Nurses. Rockville, MD: Division of Nursing, Bureau of Health Professions, Health Resources and Services Administration.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Stagg Elliott V. 2002. Public health reporting flaws spell trouble: doctors complain about requirements that appear to lack follow-through. American Medical News, April 22/29, 2002. Available online at http://www.ama-assn.org/sci-pubs/amnews/pick_02/hll20422.htm. Accessed March 14, 2003.
Starfield B. 1998. Primary Care: Balancing Health Needs, Services and Technology. New York: Oxford University Press.
Starfield B. 2002. The role of primary care in improving population health and equity in the distribution of health: an unappreciated phenomenon. Presented at the Macy-Morehouse Conference on Primary Care, Atlanta, GA, September 17–19, 2002.
Starfield B, Shi L. 2002. Policy-relevant determinants of health: an international perspective. Health Policy 60:210–218.
Strasz M, Allen DJ, Paterson Sandie AK. 2002. EPSDT: Early Periodic Screening Detection and Treatment: a snapshot of service utilization. The Michigan Council for Maternal and Child Health. Available online at www.mcmch.com/docs/EPSDT.pdf. Accessed September 29, 2002.
Sturm R, Wells K. 2000. Health insurance may be improving—but not for individuals with mental illness. Health Services Research 35(1 Pt. 2):253–262.
Sturm R, Jackson CA, Meredith LS, Yip W, Manning WG, Rogers WH, Wells KB. 1995. Mental health care utilization in prepaid and fee-for-service plans among depressed patients in the medical outcomes study. Health Services Research 30(2):319–340.
Substance Abuse and Mental Health Services Administration. 2001. SAMHSA fact sheet: analysis of alcohol and drug abuse expenditures in 1997. SAMHSA News Release. Available online at www.health.org/newsroom/releases/2001/april01/12.htm. Accessed April 16, 2002.
Teutsch SM, Churchill RE (Eds.). 1994. Principles and Practices of Public Health Surveillance. New York: Oxford University Press.
Thacker SB, Stroup DF. 1994. Future directions for comprehensive public health surveillance and health information systems in the United States. American Journal of Epidemiology 140:383–397.
Trude S, Christianson JB, Lesser CS, Watts C, Benoit AM. 2002. Employer-sponsored health insurance: pressing problems, incremental changes. Health Affairs 21(1):66–75.
University of Illinois at Chicago. 1999. Linking affordable housing to community development. University of Illinois at Chicago City Design Center, Community Design Excellence. Available online at www.uic.edu/aa/cdc/files/LinkingAffordableHousing.html. Accessed September 26, 2002.
U.S. Department of Housing and Urban Development. 2002. Building Higher Education— Community Development Corporation Partnerships. Washington, DC: Department of Housing and Urban Development.
U.S. House of Representatives. 2001. National Preparedness: Ambulance Diversions Impede Access to Emergency Rooms . Washington, DC: Special Investigative Division, Minority Staff for Representative Henry A. Waxman, Committee on Government Reform, U.S. House of Representatives.
U.S. Office of Management and Budget (OMB). 2001. Budget of the United States Government. Fiscal year 2002. Washington, DC: Government Printing Office. Available online at www.whitehouse.gov/omb/budget. Accessed March 2, 2002.
VHA Health Foundation and the AHA Health Research and Educational Trust (HRET). 2000. Sustaining community health: the experience of health care system leaders. White paper. Irving, TX: VHA Health Foundation
Viccellio P. 2001. Emergency department overcrowding: an action plan. Academic Emergency Medicine 8(2):185–187.
Wagner EH, Austin BT, Von Korff M. 1996. Improving outcomes in chronic illness. Managed Care Quarterly 4(2):12–25.
Suggested Citation:"5. The Health Care Delivery System." Institute of Medicine. 2003. The Future of the Public's Health in the 21st Century. Washington, DC: The National Academies Press. doi: 10.17226/10548.
×
Wagner EH, Austin BT, Davis C, Hindmarsh M, Schaefer J, Bonomi A. 2001. Improving chronic illness care: translating evidence into action. Health Affairs 20(6):64–78.
Wagner TH, Guendelman S. 2000. Health care utilization among Hispanics: findings from the 1994 Minority Health Survey. American Journal of Managed Care 6:355–364.
Wang PS, Berglund P, Kessler RC. 2000. Recent care of common mental disorders in the United States. Journal of General Internal Medicine 15(5):284–292.
Welch WP, Miller ME, Welch HG, Fisher ES, Wennberg JE. 1993. Geographic variation in expenditures for physician' services in the United States. New England Journal of Medicine 328:621–627.
Wells BL, Horm JW. 1992. Stage at diagnosis in breast cancer: race and socioeconomic factors. American Journal of Public Health 82(10):1383–1385.
Wells KB, Sherbourne C, Schoenbaum M, Duan N, Meredith L, Unützer J, Miranda J, Carney MF, Rubinstein LV. 2000. Impact of disseminating quality improvement programs for depression in managed primary care: a randomized controlled trial. Journal of the American Medical Association 283(2):212–220.
Woolhandler S, Himmelstein DU. 1988. Free care: a quantitative analysis of health and cost effects of a national health program for the United States. International Journal of Health Services 18(3):393–399.
Young AS, Grusky O, Jordan D, Belin TR. 2000. Routine outcome monitoring in a public mental health system: the impact of patients who leave care. Psychiatric Services 51(1):85–91.
Young AS, Klap R, Sherbourne CD, Wells KB. 2001. The quality of care for depressive and anxiety disorders in the United States. Archives of General Psychiatry 58:55–61.
Zambrana RE, Breen N, Fox SA, Gutierrez-Mohamed ML. 1999. Use of cancer screening practices by Hispanic women: analyses by subgroup. Preventive Medicine 29:466–477.
Zuvekas SH, Banthin JS, Selden TM. 1998. Mental health parity: what are the gaps in coverage? Journal of Mental Health Policy and Economics 1(3):135–146.
Zuvekas SH. 2001. Trends in mental health services use and spending, 1987–1996. Health Affairs 20(2):214–224.
Delivering Healthcare in America Chapter 8 Review Questions 6th Edition
Source: https://www.nap.edu/read/10548/chapter/7